ABSTRACT
In addition to the most likely diagnoses for umbilical signs in adults (umbilical hernia, metastatic tumour, endometriosis, congenital abnormalities such as umbilical-urachal sinus and gallstones retained or spilled at the umbilicus), the differential diagnosis should also include epidermoid cyst arising from the skin of the umbilicus. We describe the case of a young man who presented with a persistent umbilical discharge which was initially thought to be umbilical-urachal sinus, but later found to be a sebaceous cyst.
LEARNING POINTS
- Umbilical sebaceous cysts are rarebut should be included in the differential diagnosis in patients presenting with umbilical discharge, erythema, pain or a palpable mass.
- They should be considered even when the cystic lesion involves the white line, where remnants of embryonic structures are more likely, as they have been described both above and belowthe fascia, extending and penetrating the white line.
- Preoperative imaging including ultrasound as well as CT helps to differentiate between umbilical sebaceous cysts and urachal sinus, thusfacilitating adequate preoperative planning to ensure a better outcome.
KEYWORDS
Umbilicus, sebaceous cyst, urachus, urachal sinus, CT, ultrasound scan
INTRODUCTION
Various diseases such as non-neoplastic processes (umbilical hernia, endometriosis, psoriasis, hypertrophic scar, granuloma, pilonidal sinus, mycosis,eczema, sebaceous cyst and embryological remnants of the urachus and omphalomesenteric duct) and neoplastic processes (Paget’s disease, angioma and metastatic cancer)can present with umbilical pathology. Sebaceous cysts of the umbilicus are rare and reported less frequently than other conditions. However, they should be included in the differential diagnosis for cystic lesions of the umbilicus or inflammatory processes that include the umbilicus. Imaging techniques for periumbilical conditions include ultrasound and abdominal CT.
CASE REPORT
We describe the case of a 19-year-old manwho presented to the acute admissions unit of our hospital with a 1-week history of abdominal pain associated with a light green umbilical discharge. The pain was described as dull and aching and mostly localized around the umbilicus and lower abdomen. The patient had undergone a 5-day course of oral flucloxacillin with no improvement in his symptoms. He was otherwise fit and well and there was no medical history of note.
On physical examination, the patient appeared generally well. He was haemodynamically stable and apyrexial. On abdominal examination, he had a soft abdomen with mild tenderness mostly around the umbilicus. An umbilical discharge of a light green fluid was noted, but no erythema or signs of cellulitis were seen.Initial laboratory findings were Hb15.6, WCC 8.3 and CRP 11.6. A urine dipstick was unremarkable.
The patient underwent a preoperative abdominopelvic ultrasound scan (USS) which demonstrated a 1.7×2.4cm hypoechoic focus just deep to the linea alba/anterior abdominal wall in the midline, lying below the umbilicus. No collection was demonstrated within the subcutaneous compartment (Fig. 1).
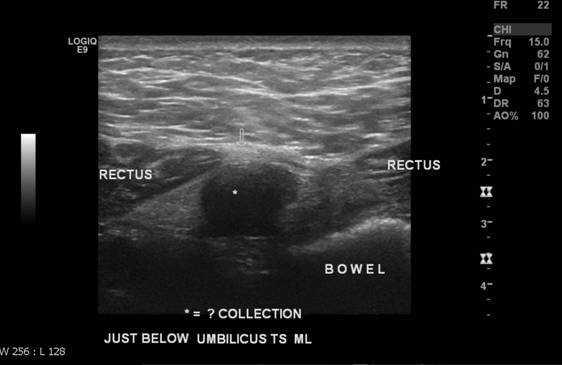
Figure 1 (click to enlarge)
Figure 1. Anterior abdominal wall ultrasound scan showing the sebaceous cyst
It was unclear whether this represented a small collection or a loop of small bowel adherent to the abdominal wall,so the patient underwent an abdominal CT scan to exclude an enterocutaneous fistula. The results demonstrated a thick-walled 15mm collection just deep to the umbilicus within the region of the linea alba. No associated intrabdominal collection was seen, although a little fluid deep within the right side of the pelvis was noted. There were some small bowel loops closely adjacent to the region of the collection, but nodefinite bowel wall thickening was evident and appearances were otherwise unremarkable (Fig.2). On the sagittal reconstructions, a tract running from the collection to the bladder dome was demonstrated (Fig.3). The provisional diagnosis based on the clinical and CT findings was an infected urachal sinus.


Figure 2. Axial CT scan of the abdomen showing the sebaceous cyst
Figure 3. Sagittal CT scan of the abdomen showing the sebaceous cyst
The patient proceeded to undergo incision and drainage of the umbilical collection. The intraoperative findings were an inflamed lesion containing pus and sebum extending from the skin of the umbilicus to the white line. Excision of the cyst was not possible because of the surrounding inflammation. Swabs for microbiological analysis were taken. Based on the intraoperative findings of the sebum within the lesion,the diagnosis of an inflamed umbilical sebaceous cyst extending to the linea alba, that was mimicking an infected urachal sinus, was made.
DISCUSSION
Umbilical signs in adults may be suggestive of multiple diseases. However,cystic lesions of the umbilicus generally indicate omphalomesenteric duct or urachal remnants and sebaceous cyst arising from the skin of the umbilicus. Although urachal and omphalomesenteric duct remnants are well described in the literature, sebaceous cyst of the umbilicus was first described in 1995 by Molderez et al. in a patient with umbilical discharge[1]. In 2002, McClenathan described aseries of seven patientswith a variety of clinical symptoms and signs such as pain, which was radiating in some patients away from the umbilicus, umbilical drainage, a palpable mass or erythema around the umbilicus[2]. Umbilical cyst has been also described as a complication after abdominoplasty[3] due to epidermal inclusion at the site of the umbilicus[4]. None of the patients of Molderez or McClenathan wereexamined or reported a previous operation around the umbilicus. Sebaceous cyst of the umbilicus is mostly seen in adults, but cases in later childhood, where anomalies due to failure of an embryologic process are most likely seen, have also been published[1] McClenathan reported the sebaceous cystswere mostly located above the midline fascia but also described some below the fascia with communication with the skin through a tiny fascial opening[2].
Virmani etal. concluded that a CT scan and MRI can detect the fat and cystic content within a lesion, so benign lesions such as epidermoid cysts and simple lipomas can be differentiated from their malignant counterparts[5].
The elective excision of asymptomatic umbilical sebaceous cysts is never reported and they are mostly excised when discovered as an incidental finding during examination of inflammatory processes of the umbilicus.
Our patient is the first casewhere a sebaceous cyst has been described within the linea alba extending to the umbilicus. This finding together with the existence of a urachal tract resulted in the diagnosis of an infected urachal sinus.