ABSTRACT
A 48-year-old man presented to our emergency department with neck pain without sensorimotor deficit and with a sore throat without signs of infection. Magnetic resonance imaging was performed because the patient had not responded to regular treatment and a blood test had showed inflammation. The images revealed cervical prevertebral fluid collection and calcification, compatible with acute calcific tendinitis of the longus colli muscle. Prednisolone 50 mg with pantoprazol 40 mg was administered for 5 days with rapid resolution of symptoms. Acute calcific tendinitis of the longus colli muscle is a rare and possibly underdiagnosed cause of atypical neck pain and sore throat.
LEARNING POINTS
- The signs and symptoms of acute calcific tendinitis of the longus colli muscle can easily be mistaken for serious disease such as spondylodiscitis or retropharyngeal abscess.
- Imaging with easily available modalities such as computed tomography can be used for diagnosis.
- Anti-inflammatory medication led to quick resolution of symptoms despite elevated signs of inflammation and delayed diagnosis in our patient.
KEYWORDS
Retropharyngeal swelling, prevertebral fluid collection, inflammatory neck pain
INTRODUCTION
The first report in the 1960s of acute calcific tendinitis of the longus colli muscle as a cause of neck pain was followed by a few other articles[1,2]. However, recent years have seen an increase in publications[2]. Typical signs include neck pain, a sore throat, a reduction in neck range of motion, calcification and fluid collection in the prevertebral space[2–6]. Signs and symptoms can easily be mistaken for serious disease such as spondylodiscitis, meningitis or retropharyngeal abscess. The aetiology of the condition is still unclear. Histologically, hydroxyapatite crystals are deposited in the tendon of the longus colli muscle accompanied by foreign body inflammation[6]. Treatment consists of the administration of non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids[2–5].
CASE DESCRIPTION
A 48-year-old man presented with a 3-day history of neck pain that intensified with rotation of the neck to the right. The patient had not experienced previous trauma or similar complaints within the previous 12 months. Consumption of paracetamol did not improve the pain. There were no sensorimotor deficits, fever or chills. The patient’s past medical history was unremarkable except for pollen allergy and a whiplash injury sustained in a car accident many years previously. There was no regular drug ingestion. Some of the patient’s work was physically demanding. The patient was in good general condition with normal weight, afebrile and haemodynamically stable. There was a marked paravertebral right dominant myogelosis at the cervical spine (CS) until the occiput. Reclination and rotation of the head to the right, particularly if active, was restricted although possible. Neurological examination was unremarkable. NSAIDs were prescribed, the neck was immobilized with a cervical collar and the patient was discharged.
A few days later, the patient returned with increased complaints. The pain had slowly changed character from being movement associated to slight pain at rest. Additionally, there was new low-grade odynophagia. Fever and chills were absent and the patient’s general condition was still good. However, the spinous processes were tender to palpation at the level of cervical vertebrae 2 and 3, and head rotation to the right was restricted at 5° active and 20° passive. Reclination was almost impossible due to pain. There were no sensorimotor deficits, otorhinolaryngological focus of infection or meningitis. Blood analysis showed leucocytosis of 12.4×109/l (normal range 3.5–10×109/l), elevated C-reactive protein (CRP) of 48.9 mg/l (normal value <10 mg/l) and slightly elevated gamma-glutamyl-transferase (GGT). The other results were within normal ranges.
Conventional x-ray of the CS showed no pathological findings besides degenerative changes (Fig. 1). The patient’s complaints increased despite intensified pain-relief measures. We therefore carried out magnetic resonance imaging (MRI) which revealed prevertebral fluid collection and a signal alteration suggesting calcification on the ventral side of cervical vertebrae 1 and 2. These signs were compatible with acute calcific tendinitis of the longus colli muscle (ACTLC) (Fig. 2).
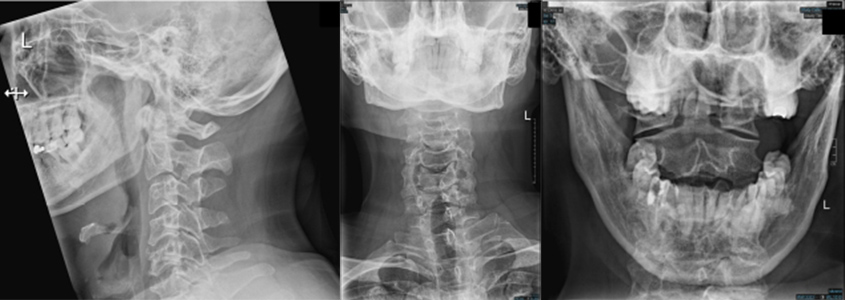
Figure 1 (click to enlarge)
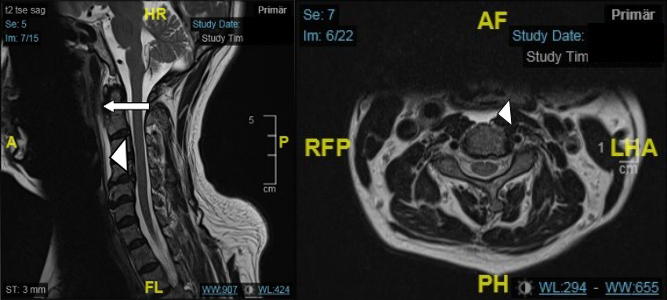
Figure 2 (click to enlarge)
Figure 1. (Left panel) X-ray of the cervical spine (CS), lateral view; (middle panel) x-ray of the CS, antero-posterior view; (right panel) x-ray of the dens axis, axial view
Figure 2.(Left panel) MRI of the cervical spine (CS), sagittal view T2 turbo spin echo (TSE); (right panel): MRI of the CS, axial view T2 TSE. Arrowhead: prevertebral fluid collection; arrow: calcification
DISCUSSION
The longus colli muscle is the deepest of the anterior neck muscles in the prevertebral space immediately posterior to the retropharyngeal space. The inflammation-related swelling of the prevertebral tissue could well explain the neck pain and sore throat of our patient. The presentation, past history of trauma and clinical and radiological findings were typical of ACTLC.
The first report of neck pain linked to retropharyngeal calcification and swelling on a conventional x-ray was published in 1964 by Hartley[1]. A steady increase in the number of similar cases since then was described in an article by Shawky et al.[2]. The authors reviewed 81 publications describing 242 patients, most of which were published between 2008 and 2015. Neck pain was reported in 100% and reduced neck mobility in 98.3%. Sore throat including dysphagia, odynophagia or globus sensation was reported in 83.7%. A CRP value was documented in 21 cases, 15 of which were within the normal range[2]. In two Korean analyses of 18 case reports, neck pain and reduced range of neck motion was found in 100% and odynophagia in 88% of cases[3,4]. Some case reports described the use of conventional x-rays, CT or MRI for diagnostic purposes. In a Danish case series, MRI in all four reported patients demonstrated prevertebral soft tissue swelling, as revealed by hyperintensity in short tau inversion recovery (STIR) sequences, and calcification anterior to cervical vertebra 1, as revealed by signal alteration in T1 sequences[5]. Suh et al. reported calcification anterior to cervical vertebra 2 and prevertebral soft tissue swelling on CT in all 10 of their patients; in eight of the patients calcification was also seen on conventional x-ray[4].
A case report from 1994 suggested the aetiology might be a foreign body reaction to hydroxyapatite crystals in the tendon of the longus colli muscle as documented in histological workup of a non-specific retropharyngeal soft tissue mass[6]. Prior trauma and upper respiratory tract infection as a cause were also hypothesized[6].
Shawky et al. reported that 55% of cases were successfully treated with NSAIDs and 22% with corticosteroids[2]. Suh et al. reported that all 10 of their patients received intravenous methylprednisolone with rapid alleviation of symptoms[4]. The eight patients in the case series of Yeong-Jin et al. all received NSAIDs and symptoms improved in 1–2 weeks[3].
CONCLUSION
ACLTC is a rare cause of neck pain. The combination of neck pain, odynophagia and reduced range of neck motion is a hallmark of this condition[1–4]. The typical radiological signs are prevertebral calcification and soft tissue swelling on CT and prevertebral fluid collection on MRI[4,5]. Previous neck trauma could be a possible cause of calcium hydroxyapatite deposition in the longus colli muscle. Treatment consists of NSAIDs and corticosteroids[2–4].