ABSTRACT
Ogilvie’s syndrome or acute colonic pseudo-obstruction is characterized by massive colon dilation in the absence of mechanical obstruction or toxic megacolon. The phenotype associated with secretory diarrhoea is rare and is related to increased potassium channel activity in the colon, inducing excessive potassium loss, with increased sensitivity to normal serum aldosterone levels. The recommended therapy is potassium-sparing agents. We present the case of an 85-year-old patient who was admitted at the emergency department with prostration, abdominal distension and diarrhoea, corresponding to functional colonic dilation precipitated by severe hypokalaemia. Resolution of the condition only occurred after spironolactone was administered for suspected primary hyperaldosteronism, which was not proved as the patient showed normal aldosterone serum levels. The pathophysiological mechanism of abnormal potassium secretion in this scenario corresponds to ‘relative hyperaldosteronism’ caused by increased sensitivity of colonocytes to aldosterone.
LEARNING POINTS
- Colonic pseudo-obstruction is not usually associated with secretory diarrhoea and severe hypokalaemia.
- Although serum aldosterone levels are normal, the treatment of choice is spironolactone due to its effect on the potassium channels in colonocytes.
- It is essential to recognize this specific phenotype so that the correct clinical approach, diagnosis and management can be established.
KEYWORDS
Ogilvie’s syndrome, colonic pseudo-obstruction, hypokalemia, spironolactone
CASE DESCRIPTION
We present the case of an 89-year-old female patient with chronic renal disease and dementia, and not taking any hypokalaemic drugs, who was admitted at the emergency department with prostration, abdominal distension and diarrhoea on previous days. The patient was found to have a distended, timpanized and tender abdomen with no signs of peritoneal irritation but with metallic bowel sounds. Laboratory tests showed severe hypokalaemia (2.1 mmol/l). Simple abdominal radiography revealed exuberant colonic dilatation (Fig. 1), while computerized tomography showed distention of the entire colon, with a maximum calibre of 85 mm, which contained liquid and had a wall of normal thickness and uptake; no mechanical obstruction, pneumoperitoneum or free intraperitoneal fluid was identified (Fig. 2 A,B). The diagnosis of Ogilvie’s syndrome in the context of severe hypokalaemia was made. The patient started oral and intravenous potassium replacement, without clinical or laboratory improvement. In the absence of other causes and due to the suspicion of hyperaldosteronism, a therapeutic test with spironolactone was performed after blood sampling for aldosterone levels, with normalization of serum potassium levels and clinical resolution of the diarrhoea and abdominal distension. Plasma levels of aldosterone were normal, which raised doubts about the diagnosis despite the evident clinical improvement after therapy.
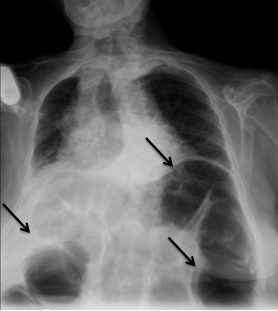
Figure 1 (click to enlarge)
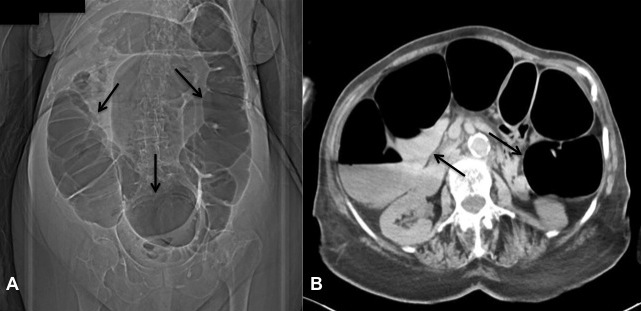
Figure 2 (click to enlarge)
Figure 1. Abdominal radiographic images showing exuberant colonic dilatation
Figure 2. Computerized tomographic images showing distention of the entire colon
DISCUSSION
Ogilvie’s syndrome or acute colonic pseudo-obstruction is characterized by massive colon dilation in the absence of mechanical obstruction or toxic megacolon[1]. Although constipation is the most common symptom, approximately 20–40% of patients may experience diarrhoea[2] and consequent hypokalaemia due to increased colonic hypersecretion of potassium[3]. This is caused by the overexpression or increased responsiveness of potassium channels in the colon, with increased sensitivity to normal aldosterone levels[1], which explains the improvement or resolution of hypokalaemia after initiation of spironolactone, as evidenced in the present case[4]. This phenotype is rare and is called acute colonic pseudo-obstruction associated with secretory diarrhoea[1]. Prospective studies are warranted to precisely describe the clinical and biological features of this phenotype of colonic pseudo-obstruction, delineate its course, and formally evaluate the therapeutic efficacy of potassium-sparing agents in its management[1].