ABSTRACT
Hemichorea is a rare clinical manifestation of type 2 diabetes mellitus. The patient presents with non-ketotic hyperglycaemia, hemichorea (characterized by rapid and involuntary movements of a specific part of the body) and the CT imaging reveals the presence of alterations involving the ganglia of the base[1-3].
LEARNING POINTS
- Hemichorea is a rare clinical manifestation of type 2 diabetes mellitus associated with an uncontrolled disease.
- Hyperglycaemic hemichorea has a good prognosis.
- All diabetics need to maintain good metabolic control and control cardiovascular risk factors.
KEYWORDS
Diabetes mellitus, hyperglycaemic hyperosmolar syndrome, hyperglycaemic hemichorea
CASE DESCRIPTION
An 86-year-old woman, with a 20-year history of type 2 diabetes mellitus (DMT2) came to the ER due to motor agitation with involuntary movements of the left upper extremity with 3 days of evolution. She was apyretic, hypotensive and dehydrated. Involuntary, irregular and non-suppressible movements of the left superior member with involvement of the ipsilateral face were noted. The patient was found to be hyperglycaemic with a serum glucose of 1,045 mg/dl and also had hyperosmolar hyponatraemia, anaemia, leucocytosis with neutrophilia, acute renal injury and elevated troponin I, with non-supraST waves on the ECG. In the urine summary, the findings were of leucocyturia without ketonuria. Hyperglycaemic hyperosmolar syndrome and hyperglycaemic hemichorea were diagnosed. A CT scan was carried out (Fig. 1) with the identification of a hyperdensity at the level of the right striatum, which corroborated the neurological findings. Infusion with insulin therapy was started, and fluid therapy, as well as other supportive care directed towards the anaemia, acute cystitis and for the acute myocardial infarction type 2, was initiated. Antipsychotic medication was also needed. At the end of 3 days of hospitalization, the patient no longer presented involuntary movements and was discharged 6 days later. The glycated haemoglobin (HbA1c) result, however, was 19.9%.
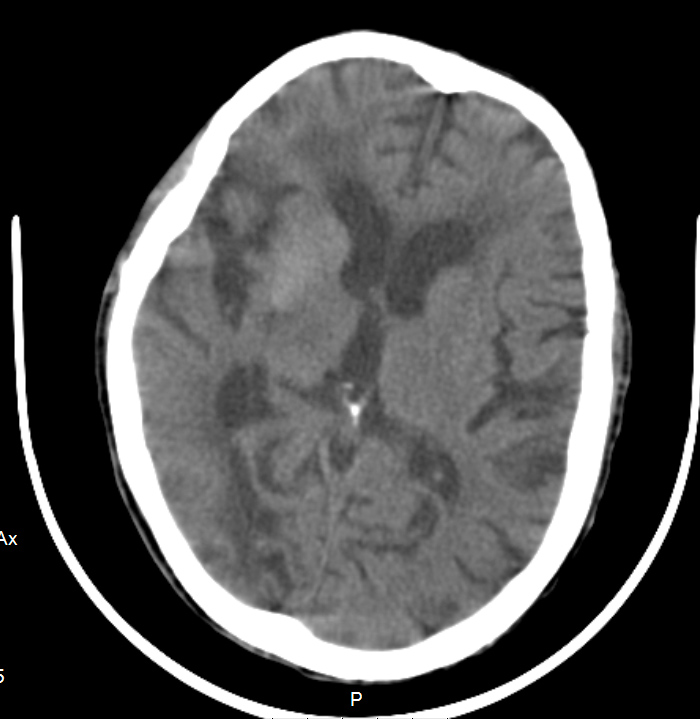
Figure 1 (click to enlarge)
Figure 1. Hyperdensity at the level of the right striatum
DISCUSSION
Most patients with hyperglycaemic hemichorea have a good prognosis, provided that they maintain good metabolic control, while therapy with dopaminergic antagonists may be necessary to control chorea[4]. This is a rare and revealing manifestation of the need for a high degree of disease control, as evidenced by the HbA1c levels in our patient.