ABSTRACT
Introduction: Idarucizumab is available for immediate reversal of dabigatran-induced anticoagulation in life-threatening bleeding or urgent surgery in patients with non-valvular atrial fibrillation (nvAF).
Case description: We report a case of an 85-year-old female treated with dabigatran for nvAF, submitted to two fast reversal procedures with idarucizumab in a 4-month period. In the first emergency episode, the patient was admitted due to a fall-related cerebral haemorrhage and subdural haematoma. There was a fast reversal of the effects of dabigatran after idarucizumab administration, which allowed stoppage of the bleeding and a decrease in intracranial pressure, with full patient recovery. Four months later, the patient revisited the hospital complaining of diffuse abdominal pain while on the same antithrombotic therapy. Physical examination showed signs of peritoneal irritation and the use of idarucizumab to reverse the effects of dabigatran was decided upon to secure normal bleeding conditions before surgery.
Discussion: Idarucizumab is an efficient, safe and feasible option for dabigatran-treated nvAF patients, when urgent anticoagulant effect reversal is needed.
LEARNING POINTS
- Clinical situations requiring urgent reversal of the anticoagulant effects of non-vitamin K antagonist oral anticoagulants are expected to be relatively rare but the existence of antidotes enables the clinical management of these situations.
- Even in independent urgent circumstances occurring over a short period of time, the repeated use of idarucizumab promptly and safely reverses the dabigatran anticoagulant effect without compromising the patient’s clinical outcome.
- The development and implementation of specific anticoagulation reversal protocols and better guidance on using baseline coagulation tests are needed to ensure timely and appropriate use of this new therapeutic option.
KEYWORDS
Atrial fibrillation, dabigatran, fast reversal, idarucizumab, urgent procedure
INTRODUCTION
Non-vitamin K antagonist oral anticoagulants (NOACs) are widely used in the prevention and treatment of stroke and thromboembolic events in patients with non-valvular atrial fibrillation (nvAF)[1].
The NOAC dabigatran etexilate is increasingly being used due to its demonstrated favourable risk–benefit profile, and also, because it was the first anticoagulant to have an approved specific reversal agent, the humanized monoclonal antibody fragment idarucizumab[2]. With a binding affinity approximately 300-fold more potent than dabigatran’s binding affinity for thrombin, it is indicated in adult patients when rapid reversal of the dabigatran anticoagulant effect is required for an emergency surgery/urgent procedure and in life-threatening or uncontrolled bleeding circumstances[3,4]. Despite the results from clinical trials, where reversal effects were evident almost immediately after administration[4], information on the use of idarucizumab in the clinical setting remains limited.
CASE DESCRIPTION
On July 2016, an 85-year-old female patient was admitted to the emergency department due to a fall-related cerebral haemorrhage and subdural haematoma.
The patient was under anticoagulation therapy with dabigatran 110 mg due to nvAF since 2013. Past medical history included dyslipidaemia, treated with simvastatin 40 mg, and hypertension, treated with perindopril 5 mg and nebivolol 5 mg. For gastric protection, the patient was prescribed omeprazole 20 mg.
On physical examination, the patient was alert and oriented. Blood pressure (BP) was 130/80 mmHg, heart rate 72 beats/min and oxygen saturation 98%; temperature and pulmonary auscultation were normal. The patient presented 15 points on the Glasgow Coma Scale and the blood analysis showed an unaltered haemogram and renal function.
A brain computed tomography (CT) scan showed a subdural haematoma as a result of the head trauma. A fast reversal of the effects of dabigatran was required to stop the bleeding and decrease the intracranial pressure.
According to the patient, the last dose of dabigatran was taken at 8:00h of that day. After the administration of 5 g (2 x 2.5 g/50 ml) idarucizumab, there was a reversal of the coagulation markers (Table 1). Bleeding was controlled, the patient clinical situation remained stable, and anticoagulation was restarted after resorption of the subdural haematoma.
Four months later, on November 2016, the same patient was admitted to the emergency department due to diffuse abdominal pain.
Physical examination showed signs of peritoneal irritation, BP was 114/54 mmHg, heart rate 70 beats/min, oxygen saturation 96%, temperature 37.1ºC and pulmonary auscultation was normal. The medication was the same as before.
An abdominal CT scan revealed intestinal occlusion with surgical indication, and again, an urgent need to reverse the effects of dabigatran. The patient’s coagulation parameters were successfully reversed after the administration of 5 g (2 x 2.5 g/50 ml) idarucizumab, allowing the patient to be submitted to surgical treatment (Table 1).
Although no haemorrhagic complications occurred, the patient had a complicated post-operative period within the Intensive Care Unit, and died one month later.
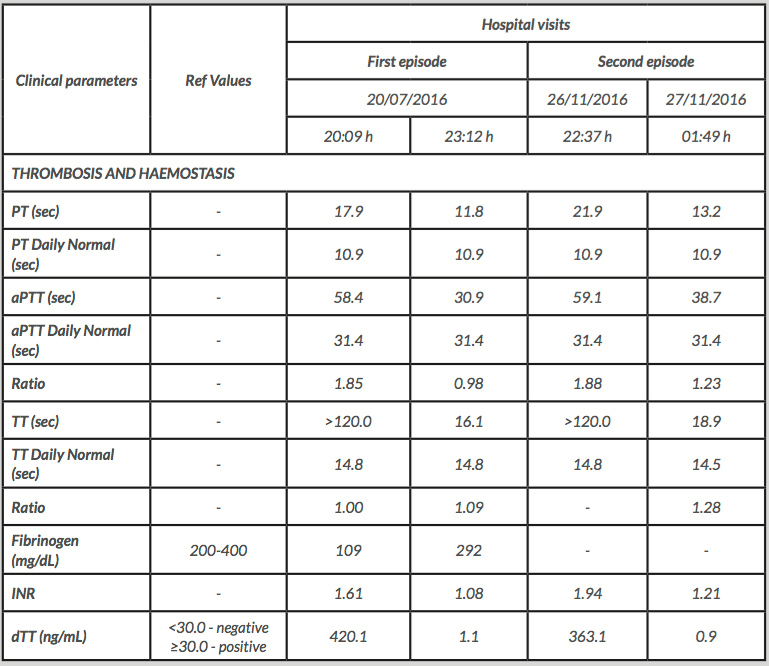
Table 1 (click to enlarge)
Table 1. Laboratory analyses: thrombosis and haemostasis.
PT - Prothrombin Time; aPTT - Activated Partial Thromboplastin Time; TT - Thrombin Time; dTT - Dabigatran diluted Thrombin Time
DISCUSSION
For more than 50 years, warfarin and other vitamin K antagonists (VKAs) were the only oral anticoagulants available for thromboembolic disease[1,2]. However, they require frequent monitoring and dose adjustments, carrying substantial risk and inconvenience[1,2]. With a favourable benefit–risk profile compared to VKAs, NOACs are presently the standard of care for stroke prevention in nvAF patients[1].
Dabigatran has demonstrated efficacy and safety in several large clinical trials and observational studies, offering potential advantages over VKAs and fewer drug interactions[1]. However, due to the lack of a reliable reversible agent that allowed an effective management of patients in emergency situations, there was some reluctance to use it. With the approval of idarucizumab, which entirely reverses the dabigatran anticoagulant effects within minutes, this situation has been overcome[2–4].
In the RE-VERSE AD trial, involving patients with life-threatening bleeding or who needed urgent invasive procedures, idarucizumab promptly reversed the effect of dabigatran[3], corroborating its role in improving patient safety in a variety of situations requiring the rapid reversal of the anticoagulant effect. Moreover, idarucizumab has been associated with an effective haemeostasis in the setting of several emergency high-bleeding-risk surgeries or invasive procedures (see Appendix).
Nevertheless, clinical situations requiring urgent reversal of the anticoagulant effects of NOACs are expected to be relatively rare[1]. The incidence of major bleeding events is significantly reduced with NOACs compared to VKAs, and treatment discontinuation (along with supportive measures) are often sufficient, even in patients with moderate-to-severe bleeding[1,2].
Despite the recommendation that emergency interventions or procedures should not be performed until at least 12h (and ideally 24h) after the last NOAC dose intake, to reduce the risk of bleeding complications[1], the reversal of the effects of dabigatran by idarucizumab was successful in the two independent emergency situations reported in our real-life clinical case.
In a Phase I study, an idarucizumab 5 g intravenous infusion was administered a second time to a subgroup of six healthy subjects to study the presence of anti-idarucizumab antibodies two months after the first administration. No idarucizumab antibodies were detected before the second administration, and afterwards they were only detected in one subject[5]. No impact on idarucizumab pharmacokinetics or reversal effects was observed, which makes it possible to predict that haemeostasis is effectively achieved without affecting patient safety in similar settings.
The specific roles of antidotes, when used with direct oral anticoagulants in reducing case fatality or improving the overall clinical course of these events, are not thoroughly understood. The development and implementation of specific anticoagulation reversal protocols and further knowledge of real-world-experience data are needed for the optimal reversal of dabigatran anticoagulation effects in emergency situations.
Our case report provides additional evidence regarding the efficiency, safety and feasibility of idarucizumab in the emergency setting for dabigatran-treated patients with nvAF when an urgent reversal is needed.