ABSTRACT
A 20-year-old Swiss male presented at the emergency department with acute onset of febrile temperatures and hemoptysis and a 3-month history of productive cough. An X-ray and CT scan of the chest, sputum samples for acid-fast bacilli, polymerase chain reaction(PCR), and cultures for Mycobacteria revealed pulmonary infection with Mycobacterium tuberculosis. None of the classical risk factors for tuberculosis were present, but the patient reported regularly smoking a water pipe. Water-pipe smoking poses a serious risk of M. tuberculosis transmission.
LEARNING POINTS
- This case report illustrates an unusual risk factor for tuberculosis: water-pipe smoking.
- With the higher social acceptance of water-pipe smoking, physicians must be aware of the associated complications.
KEYWORDS
Mycobacterium tuberculosis, risk factors, water-pipe smoking, transmission, infection, cavern
INTRODUCTION
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis. It is still one of the top 10 causes of death worldwide, and thus remains a global health threat. In 2017, there were 1.6 million deaths due to TB infections, including among HIV-positive individuals. Although TB is a global disease with as many as 10 million people infected in 2017, two thirds of affected patients live in just eight countries, i.e., India (27%), China (9%), Indonesia (8%), the Philippines (6%), Pakistan (5%), Nigeria (4%), Bangladesh (4%) and South Africa (3%)[1]. With increasing migration, the appearance of TB in high-income countries is expected to become more common. Therefore, physicians need to be alert to M. tuberculosis infections and aware of unusual risk factors for the condition.
CASE REPORT
A 20-year-old Swiss male reported a three-month history of productive cough. After febrile temperatures for several days, he experienced hemoptysis, which prompted him to visit the emergency unit. Apart from these symptoms, the patient’s medical history was unremarkable. He did not take any medication.
On admission, his temperature was raised (38.3°C), but the remainder of his physical examination was unremarkable. A chest X-ray showed a pulmonary infiltrate in the left upper lobe (Fig. 1). Computed tomography (CT; Fig. 2) examination of the lungs revealed several cavernous lesions. Sputum samples were negative for acid-fast bacilli, but PCR for M. tuberculosis complex was positive. Cultures grew M. tuberculosis with low-level isoniazid monoresistance.
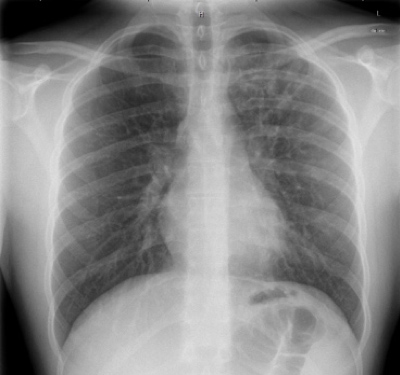
Figure 1 (click to enlarge)
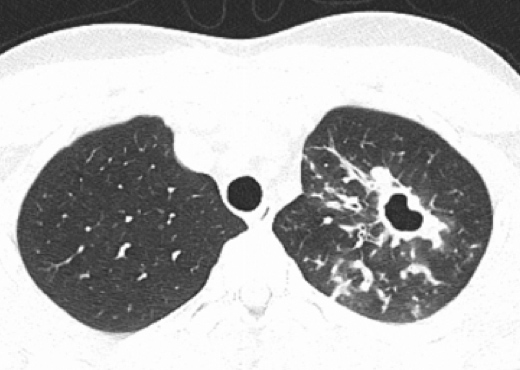
Figure 1 (click to enlarge)
Figure 1. Chest X-ray with infiltrate in the left upper lobe
Figure 2. CT scan shows a cavern in the left upper lobe, one of multiple throughout the lung
A 4-agent tuberculosis treatment (isoniazid, ethambutol, pyrazinamide and rifampicin) was given for 2 months, followed by a 4-month treatment regimen with isoniazid, rifampicin and moxifloxacin because of the low-level isoniazid monoresistance. The patient received the medication according to the directly observed treatment (DOT) approach.
None of the classical risk factors for tuberculosis were present. The patient had travelled to England, Spain and Dubai in the previous 2 years but had no known exposure to tuberculosis. Furthermore, there was nothing to point to an immune difficiency, such as HIV infection, malnutrition or drug abuse. However, the patient reported regularly smoking a water pipe (up to five days a week), usually together with the same four friends, but also in other settings. Water-pipe smoking is a previously documented source of tuberculosis transmission[4].
We were unable to identify the source of the M. tuberculosis, and no other active tuberculosis cases were found through contact investigations conducted by the Swiss pulmonary league (“Lungenliga”) and the hospital hygiene team.
DISCUSSION
Water-pipe smoking has gained popularity in the last decade. It carries risks of several diseases – chronic obstructive pulmonary disease (COPD), cardiovascular disease and cancer –, and is also associated with increased rates of infections due to M. tuberculosis[2], spore-producing fungi, herpes and hepatitis viruses[3].
The practice of sharing a water-pipe mouthpiece poses a serious risk of transmission of M. tuberculosis[2]. The number of puffs and the volume inhaled during a water-pipe smoking session are about 10 times higher than when smoking a cigarette, resulting in marked exposure to the bacteria. M. tuberculosis is a microaerophilic mesophile (between 20-45°C), making the water inside the glass base/water container (Fig. 3) an ideal habitat for the bacteria, resulting in proliferation[4]. Furthermore, in vitro data show that smoke condensate increases internalization of Mycobacterium bovis by type II alveolar epithelial cells[5].
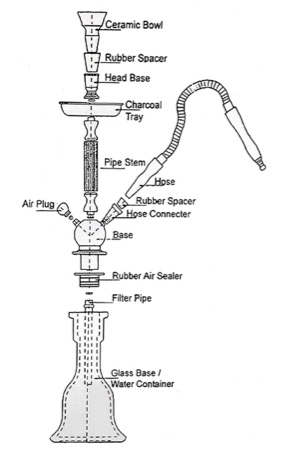
Figure 3 (click to enlarge)
Figure 3. Schematic construction of a water pipe
CONCLUSION
Our case emphasizes that water-pipe smoking is a possible risk factor for TB[3]. Physicians must ask patients about water-pipe smoking habits if TB is suspected. If TB is confirmed, all individuals who shared the water pipe must be contacted, and all water pipes involved must be destroyed.