ABSTRACT
Objectives: Baricitinib is an orally active Janus kinase (JAK) inhibitor used in the treatment of moderate to severe rheumatoid arthritis (RA).
Materials and methods: Here, we report the case of a 56-year-old Caucasian male diagnosed with RA who developed palmoplantar pustulosis (PPP) while being treated with baricitinib.
Results: The patient’s PPP resolved after discontinuation of baricitinib and recurred when this was restarted. Based on causality assessment, it was considered a drug-induced PPP.
Conclusion: To the authors’ knowledge, this is the first case of baricitinib-induced PPP.
LEARNING POINTS
- Baricitinib is a small, orally active molecule that inhibits JAK-1 and JAK-2, which is used in the treatment of rheumatoid arthritis.
- Baricitinib has been also used in the treatment of psoriasis, alopecia areata and atopic dermatitis.
- Palmoplantar pustulosis is a rare cutaneous side effect of baricitinib
KEYWORDS
Palmoplantar pustulosis, baricitinib, rheumatoid arthritis, cutaneous side effects
INTRODUCTION
Baricitinib is an orally administered, small-molecule JAK-1 and -2 inhibitor that is used in the treatment of rheumatoid arthritis (RA)[1]. Here, we report the first known case of palmoplantar pustulosis (PPP)-like eruption following baricitinib treatment for RA.
CASE DESCRIPTION
A 56-year-old Caucasian male was diagnosed with seropositive erosive RA 7 years previously. His past medical history was otherwise unremarkable. He had been treated with multiple disease-modifying antirheumatic drugs (DMARDs), including methotrexate and leflunomide. In 2014, after failure of the aforementioned DMARDs, he was started on oral baricitinib 4 mg once daily, which he was stable on for 5 years. Five years after having started baricitinib, he developed hyperkeratosis, fissuring and pustules on both palms and soles. A dermatology referral was made at that point. Clinical examination revealed thickened scaly skin with pustules on both the palms and soles (Fig. 1). The histology of a skin biopsy from the affected areas was in keeping with palmoplantar pustular psoriasis (Fig. 2).

Figure 1 (click to enlarge)
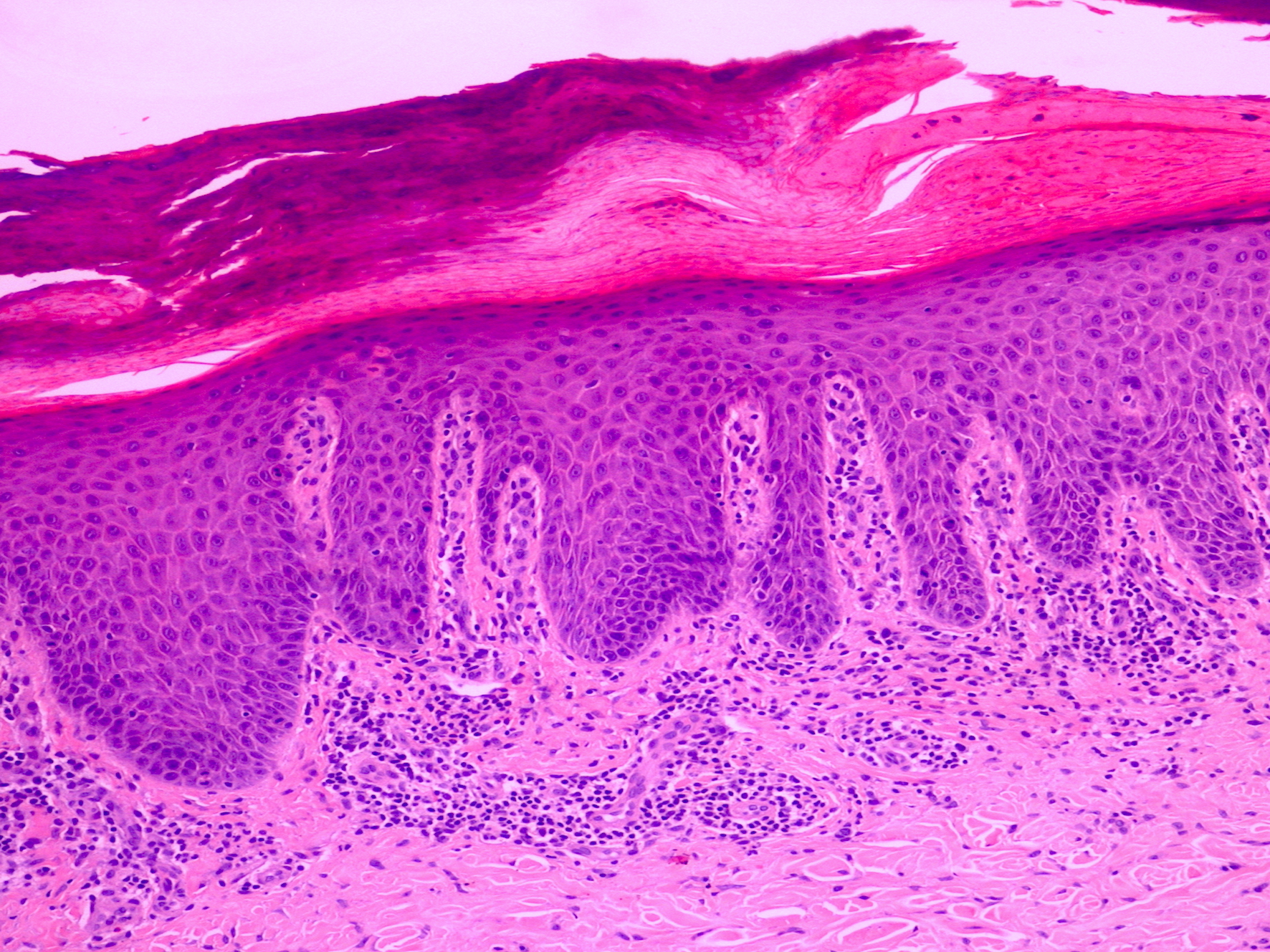
Figure 2 (click to enlarge)
Figure 1. Pustules on the affected palms
Figure 2. Histology of the skin biopsy revealed confluent parakeratosis, acanthosis, neutrophils in stratum corneum and a dermal infiltrate of lymphocytes (haematoxylin and eosin stain, x20 magnification).
The patient was seen by a dermatologist who suspected palmoplantar pustular psoriasis based on clinical and histologic findings. There was no past medical history nor family history of psoriasis or atopic dermatitis. Baricitinib was discontinued for 2 months to rule out its aetiological involvement in the palmoplantar pustular psoriasis. The patient was also prescribed topical treatment with emollients to apply twice daily and topical clobetasol propionate 0.05% ointment to use twice daily for 14 days and then every other day for 2 more weeks. After 2 months of follow-up, there was an improvement of the patient’s skin condition with near complete clearance. However, because of deterioration of his RA, baricitinib 4 mg once daily was restarted. Subsequently, the PPP reappeared on both his palms and soles after 14 days. Based on the clinical course of events, we diagnosed PPP-like eruption due to baricitinib treatment. Baricitinib dosage was lowered to 2 mg once daily, which was more tolerable for his skin condition. The patient remains under dermatology and rheumatology long-term follow-up.
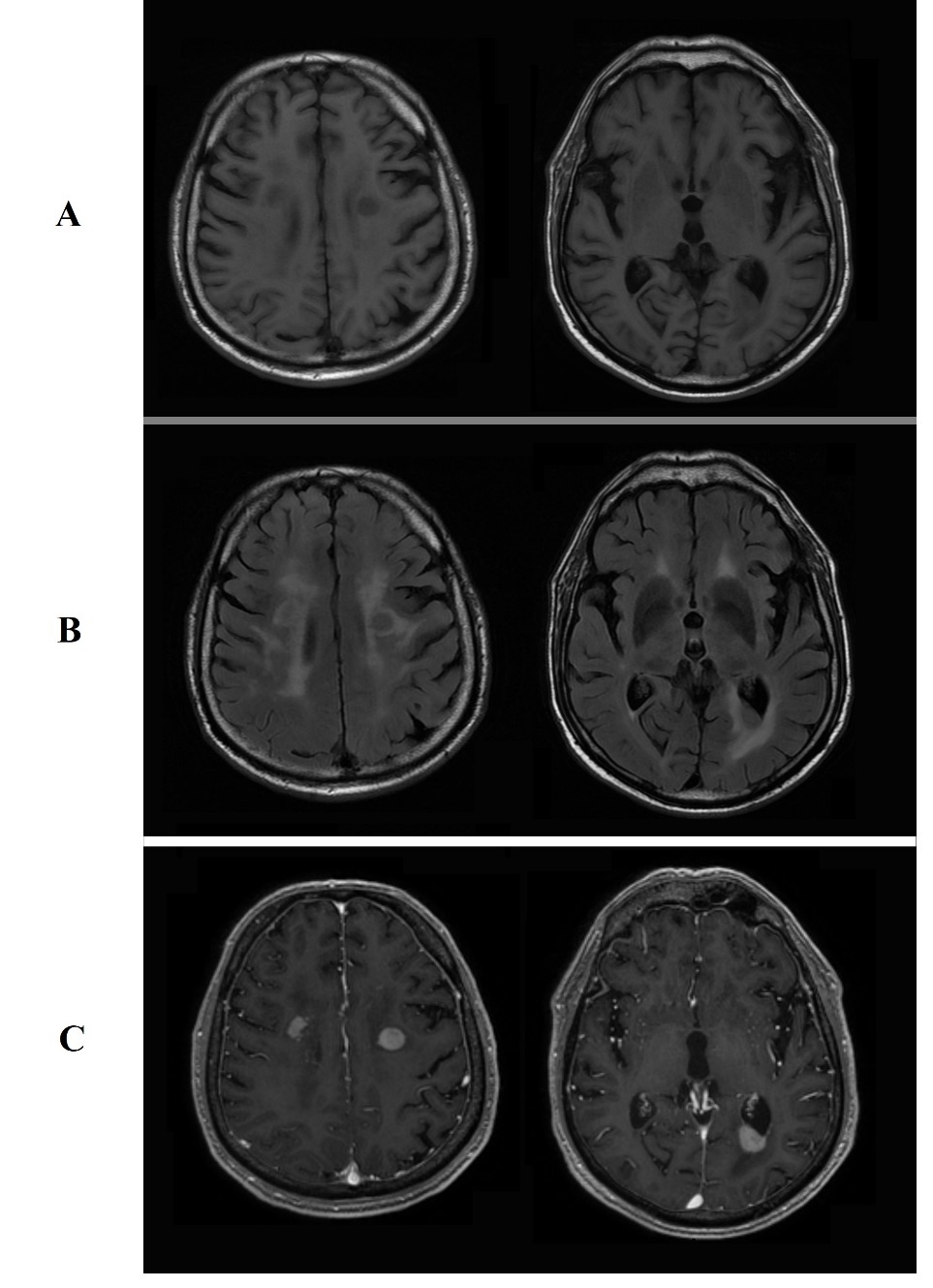
Figure 2 (click to enlarge)
Figure 2. Brain MRI lesions showing: A, hypodensity on T1-weighted images. B, isodensity on T2-weighted images. C, enhancement after gadolinium administration.
DISCUSSION
Baricitinib is a small, orally active drug available in the United States (2 mg/day), the European Union (2 and 4 mg/day) and other countries, that preferentially inhibits JAK-1 and JAK-2[1]. It is indicated for the treatment of moderate to severe active RA in adult patients who have responded inadequately to, or who are intolerant to, 1 or more DMARDs[1]. It has also been used in clinical trials for the treatment of atopic dermatitis and psoriasis[1]. Other JAK inhibitors such as tofacitinib, a JAK-1/3 inhibitor, are actually used in the treatment of PPP rather than causing disease[2,3]. Recently, a case was published regarding tofacitinib causing PPP[4]. It is well established that TNF-α inhibitors can cause PPP as a paradoxical effect. In our case, based on the clinical course of events, baricitinib was the cause of PPP. The underlying pathophysiology of this reaction is uncertain; psoriasis is thought to develop secondary to an abnormal T cell response where several cytokines are implemented such as IL-12, IL-17 and IL-23[5]. These have been shown to activate the JAK/STAT pathway[5]. IL-23 is closely associated with JAK-2[5]. JAK-1/3 inhibition may downregulate IL-1 and IL-8, which are potential mediators of PPP[3]. In conclusion, more studies investigating the pathways involved in PPP need to be carried out, including baricitinib-induced PPP and the effects of the drug on the T cell-mediated immune response.
This case highlights a new side effect of baricitinib, a JAK inhibitor, namely PPP-like eruption.