ABSTRACT
Chiari I malformation and atlanto-occipital assimilation are both fairly uncommon conditions. Symptoms usually present during adolescence or adulthood, typically consisting of headache or neck pain. Cough-associated syncope is an unusual presenting symptom. The diagnosis of this condition in a pulmonology department is even rarer.
We report the case of a 62-year-old male referred to our pulmonology department due to complaints of cough-associated syncope. After several examinations, a pharyngeal CT scan incidentally showed low positioning of the cerebellar tonsils. Cerebral MRI confirmed the diagnosis of Chiari I malformation and atlanto-occipital assimilation and the patient was effectively treated with surgical decompression.
LEARNING POINTS
- Chiari I malformation (CMI) and atlanto-occipital assimilation are both fairly rare conditions. The prevalence of CMI is estimated to range between 1/1,000 to 1/5,000 individuals and the incidence of atlanto-occipital assimilation varies from 0.08 to 3.6%.
- The most frequent clinical presentation is a paroxysmal headache or neck pain. Cough syncope is an unusual form of presentation, described in few cases.
- It is important to bear CMI in mind in the differential diagnosis of cough syncope, since there is an effective treatment that improves the patient’s symptoms and quality of life.
KEYWORDS
Cough, syncope, Chiari I malformation, atlanto-occipital assimilation
INTRODUCTION
Chiari I malformation (CMI) is characterized by a downward displacement of the cerebellar tonsils. In 23 to 45% of cases, skeletal abnormalities are also present. Atlanto-occipital assimilation refers to the congenital fusion of the atlas with the base of the occipital bone. Both of these conditions are relatively uncommon. The most frequent clinical presentation is a paroxysmal headache or neck pain. Syncope is an unusual form of presentation.
We report the case of a 62-year-old male who presented to our pulmonology department with cough-associated syncope. CMI and atlanto-occipital assimilation were diagnosed and treated with surgical decompression.
CASE DESCRIPTION
A 62-year-old Caucasian male was referred to our pulmonology department due to a 1-year history of recurrent episodes of syncope associated with cough during viral respiratory infections. He also complained of episodic occipital headaches and neck pain that responded to standard anti-inflammatory agents. He denied other respiratory symptoms, palpitations, thoracic pain or constitutional symptoms.
He had never smoked and his past medical history included hypertension and hyperlipidaemia, treated with valsartan 80 mg OD and simvastatin 20 mg OD.
Prior to referral to the pulmonary medicine, the patient underwent a thorough cardiological investigation with an electrocardiogram, echocardiogram and 24-hour Holter monitoring, all of which were normal.
The physical examination, including neurologic examination, was unremarkable.
The patient’s pulmonary function tests and chest CT scan showed no relevant changes.
Further investigation, including a paranasal and pharyngeal CT scan, was carried out. These scans incidentally revealed, besides signs of chronic rhinosinusitis, low positioning of the cerebellar tonsils through the foramen magnum (Fig. 1), suggesting Chiari malformation.
Cerebral MRI was performed to confirm the diagnosis, which revealed a partial occipitalization of the C1 vertebra with inferior cerebellar tonsillar herniation measuring 8 mm below the foramen magnum (Fig. 2). The patient was diagnosed with CMI and atlanto-occipital assimilation.
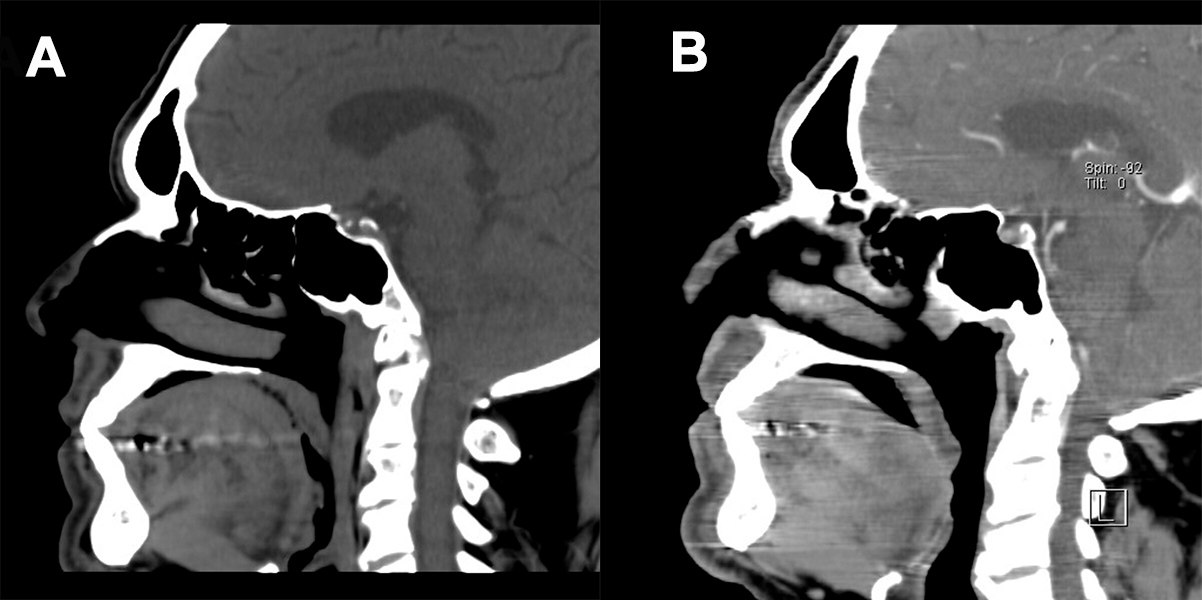
Figure 1 (click to enlarge)
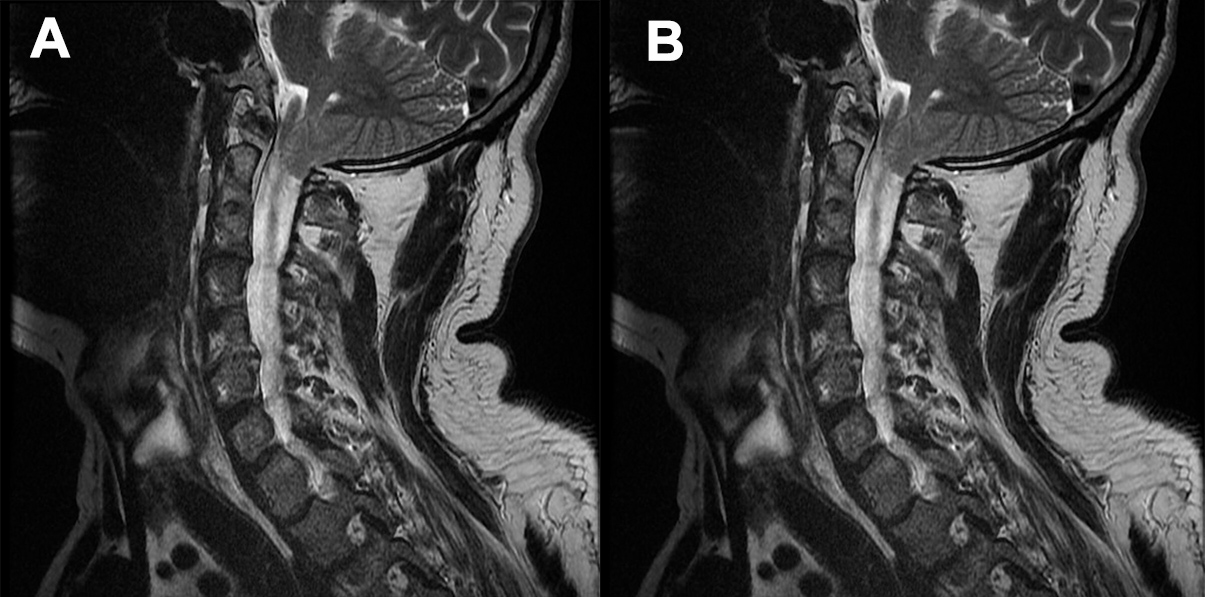
Figure 2 (click to enlarge)
Figure 1. Pharyngeal CT scan showing low positioning of the cerebellar tonsils through the foramen magnum
Figure 2. Cerebral MRI showing inferior cerebellar tonsillar herniation through the foramen magnum
He was subsequently referred to the neurosurgery outpatient clinic, where he was submitted to decompression surgery consisting of a suboccipital craniotomy, removal of the C1 posterior arch and duraplasty, with clinical improvement. After surgery, the patient denied further syncopal episodes and reported improvement of his occipital and neck pain.
DISCUSSION
Cough-associated syncope may constitute a clinical challenge given the multitude of potential pathophysiological mechanisms and different aetiologies. Possible causes may include diseases of the central nervous system, respiratory or cardiovascular systems. Although it is not uncommon for patients with CMI to present with respiratory complaints, cough syncope is a rare presenting symptom[1].
Chiari malformations are defined by anatomic anomalies of the craniocervical junction with downward displacement of the cerebellar structures[2]. These are rare conditions, classified into 6 different groups, with the most common types being Chiari I and II malformations[3].
CMI is characterized by a downward displacement of the cerebellar tonsils, 5 mm or more below the foramen magnum[2]. In 23 to 45% of cases, skeletal abnormalities are also present, namely: atlanto-occipital assimilation, such as in the presented case, platybasia, basilar invagination and so on[4]. Atlanto-occipital assimilation refers to the congenital fusion of the atlas with the base of the occipital bone and it may be complete or partial[5]. They are both relatively rare conditions. The prevalence of CMI is estimated to range between 1/1,000 to 1/5,000 individuals and the incidence of atlanto-occipital assimilation varies from 0.08 to 3.6%[1].
CMI is generally asymptomatic until adolescence or adulthood. The most frequent clinical presentation is a paroxysmal headache or neck pain. Less common presentations include sensorimotor dysfunction, lower cranial nerve palsies, nystagmus, vertigo, ataxia, dysphagia and syncope[1,2]. Syncope is a relatively rare symptom of CMI, which has been reported in a few cases. Various pathophysiological mechanisms have been proposed, such as compression of the midbrain ascending reticular system or vascular compromise. However, the exact cause is still not well understood[6].
The diagnosis of Chiari malformations is based upon neuroanatomy. Cerebral MRI is the best imaging examination modality for evaluation and diagnosis of this condition[2].
Treatment depends upon the nature of the malformation and the presence of symptoms. Asymptomatic patients may be treated conservatively with clinical and imaging surveillance. However, symptomatic patients should be surgically treated. Decompression surgery should be offered to symptomatic patients since postoperative improvement or stabilization of symptoms have been reported in the majority of patients[2].
We present a case of an uncommon central nervous system condition with a rare clinical presentation. Due to cough complaints, the patient was referred to our pulmonology department and the unexpected diagnosis of a neurological condition was made by our pulmonology team. It is important to remember CMI in the differential diagnosis of cough-associated syncope given that there is an effective treatment that improves the patient's symptoms and quality of life.