ABSTRACT
Right-sided Bochdalek hernia (BH) is very rarely diagnosed in adults. It commonly presents with gastrointestinal symptoms (pain, abdominal distension and vomiting). Breathlessness, recurrent chest infections and other pulmonary sequelae can also be present. We report the case of a 92-year-old man with a 3-day history of dyspnoea, fever and thoracic pain and multiple episodes of vomiting. An x-ray was performed, and the diagnosis of a large BH hernia was confirmed by computed tomography of the thorax. The condition may be fatal in cases where the small bowel undergoes necrosis or perforation. An emergent laparotomy was performed, but the patient did not improve clinically and died immediately after the procedure.
LEARNING POINTS
- Right-sided Bochdalek hernia (BH) is very rarely diagnosed in adults.
- Misdiagnosis of BH as a tension pneumothorax (which has a similar clinical presentation) can delay treatment and put patients at risk.
- The outcome of BH depends on the presentation, early diagnosis and emergent intervention.
KEYWORDS
Bochdalek hernia, dyspnoea
CASE DESCRIPTION
A 92-year-old man with history of chronic obstructive pulmonary disease (COPD) and hypertension was admitted to our emergency room with a 3-day history of dyspnoea, fever and thoracic pain. He denied previous trauma. On physical examination, the patient was lucid, but with abolition of breath sounds over the right hemithorax and a tender abdomen in the right upper quadrant. His blood pressure was 90/42 mmHg, heart rate was 98 bpm, respiratory rate was 30 per minute and oxygen saturation was 80% on room air. During his stay in the emergency room the patient experienced multiple episodes of vomiting which did not respond to antiemetic therapy.
Blood tests revealed a raised white cell count of 13.2×109 g/l (normal range 4–11×109 g/l) and a serum C-reactive protein of 83.5 mg/l (normal range <3.0 mg/l). Arterial blood gas analysis showed hypoxaemia (pO2 of 35 mmHg) and a lactic acid level of 4 mg/dl (normal range <2 mg/dl). Due to suspicion of pneumothorax, a chest x-ray was performed (Fig. 1) and demonstrated a large radiolucent area in the right hemithorax but with the presence of an air–fluid level. To clarify the diagnosis, computed tomography (CT) of the thorax was performed (Fig. 2) and revealed a large right posterior diaphragmatic hernia containing a segment of colon with an increased calibre of 93 mm, compatible with a large BH, which was not known previously. An emergency laparotomy was performed, but the patient did not improve clinically and died immediately after the procedure.

Figure 1 (click to enlarge)
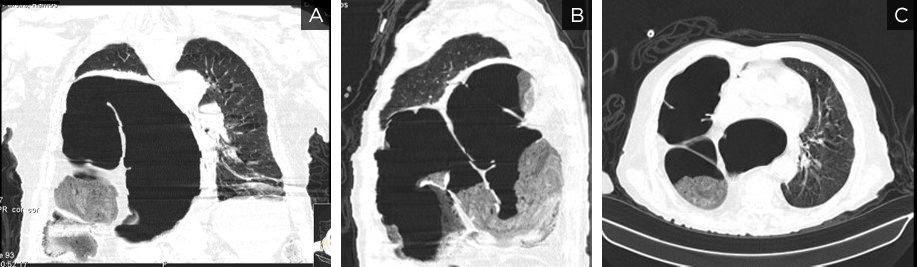
Figure 2 (click to enlarge)
Figure 1. Chest x-ray demonstrated a large radiolucent area in the right hemithorax with the presence of an air–fluid level.
Figure 2. Computed tomography of the thorax demonstrated a large right posterior diaphragmatic hernia containing a segment of colon with an increased calibre of 93 mm areas
The patient was urgently referred to the vascular surgery department and underwent an exploratory laparotomy. However, the rupture was uncontrollable and she died following cardiac arrest secondary to hypovolaemic shock.
DISCUSSION
BH occurs when the diaphragm fails to close posteriorly during embryogenesis [1]. The majority of congenital BH cases are diagnosed in childhood. There are approximately 150 reports of adult BH in the literature, but the majority of these are incidental. The incidence of BH is 0.17% in the adult population, with occurrence on the right side extremely rare because the right pleuroperitoneal canal closes earlier and the liver buttresses the right hemidiaphragm [2]. BH commonly presents with gastrointestinal symptoms (pain, abdominal distension and vomiting); breathlessness, recurrent chest infections and other pulmonary sequelae may be present, but are less common than gastrointestinal complications.
The diagnosis can be made using several imaging modalities, such as x-rays, but the condition can masquerade as a tension pneumothorax. The gold standard for diagnosis is a chest CT which has better sensitivity for left-sided hernias (78%) than right-sided hernias (50%) [3].
The condition may be fatal if the small bowel undergoes necrosis or perforation. Therefore, urgent surgical intervention is required to prevent serious complications.
In conclusion, adult presentation of right-sided BH is extremely rare and outcome depends on presentation, early diagnosis and emergent intervention.
Although rare and typically associated with childhood, these diseases can in exceptional cases be present in adult life, since a combination of some characteristics may allow children to survive. Their diagnosis is challenging in adults as they can easily be mistaken for more common diseases. However, an early diagnosis is extremely important because it allows a close follow-up and a consequent timely detection and treatment of complications, such as pulmonary infections and hemoptysis, but especially pulmonary hypertension.