ABSTRACT
A 40-year-old man presented to the emergency room and was evaluated in the internal medicine department for unexplained weight loss, asthenia, anorexia and night sweats over the previous 2 months. After a loculated pleural effusion was identified on thoracic computed tomography, purulent fluid was drained from the lung and Fusobacterium nucleatum was isolated. The patient was successfully treated for 27 days with amoxicillin-clavulanic acid. This was an atypical presentation of a common micro-organism implicated in lung infections.
LEARNING POINTS
- Empyema due to Fusobacterium nucleatum can have an atypical presentation, manifesting only with unexplained weight loss and night sweats.
- F. nucleatum lung infection usually responds well to treatment with common antibiotics.
- In patients with unexplained weight loss, the differential diagnosis should include cancer, tuberculosis and atypical presentations of other bacterial infections.
KEYWORDS
Fusobacterium nucleatum, empyema, unexplained weight loss
CASE DESCRIPTION
We present the case of a 40-year-old man who works in a cardboard factory. He has smoked 10 cigarettes a day since the age of 18. He was referred to an internal medicine consultation because of a 2-month history of an unexplained 9 kg weight loss with asthenia, anorexia and night sweats without fever or chest pain. He did not report recent contact with tuberculosis.
Physical examination revealed pale skin and cachexia. The oral cavity did not show any evidence of erosions, periodontitis, tooth loss or recent surgery. The patient was eupnoeic but had no vesicular breath sounds in the lower two-thirds of the left hemithorax and grade I splenomegaly. The rest of the physical examination was normal.
Blood analysis showed 10 410 leukocytes/μl (75.1% neutrophils, 15.8% lymphocytes), haemoglobin 11.1 g/dl, mean corpuscular volume 82.4 fl, erythrocyte sedimentation rate 37 mm, alkaline phosphatase 279 IU/l, ferritin 728 ng/ml, ultra-sensitive C-reactive protein >10 000 mg/dl, and elevation of alpha-1/alpha-2 globulins. Chest radiography demonstrated loss of volume in the left hemithorax with a probable extrapulmonary mass projecting into the upper segment of the inferior left lobe and associated pleural effusion (Fig. 1). Thoracic computed tomography showed a cystic lesion compatible with loculated pleural effusion in the left hemithorax (Fig. 2). Diagnostic thoracentesis removed approximately 100 ml of foul-smelling pus. Culture revealed multi-sensitive Fusobacterium nucleatum. Blood cultures were negative. A pleural drainage tube was placed, with instillation of urokinase and treatment with amoxicillin-clavulanic acid for 27 days, with good evolution (Fig. 3).
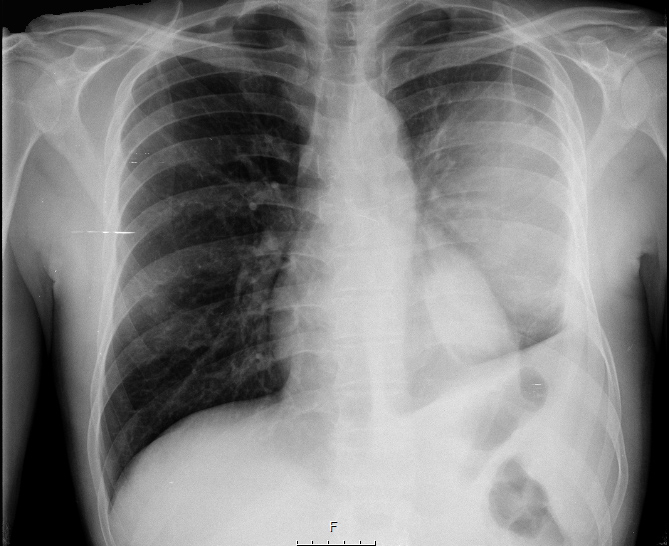
Figure 1 (click to enlarge)

Figure 2 (click to enlarge)
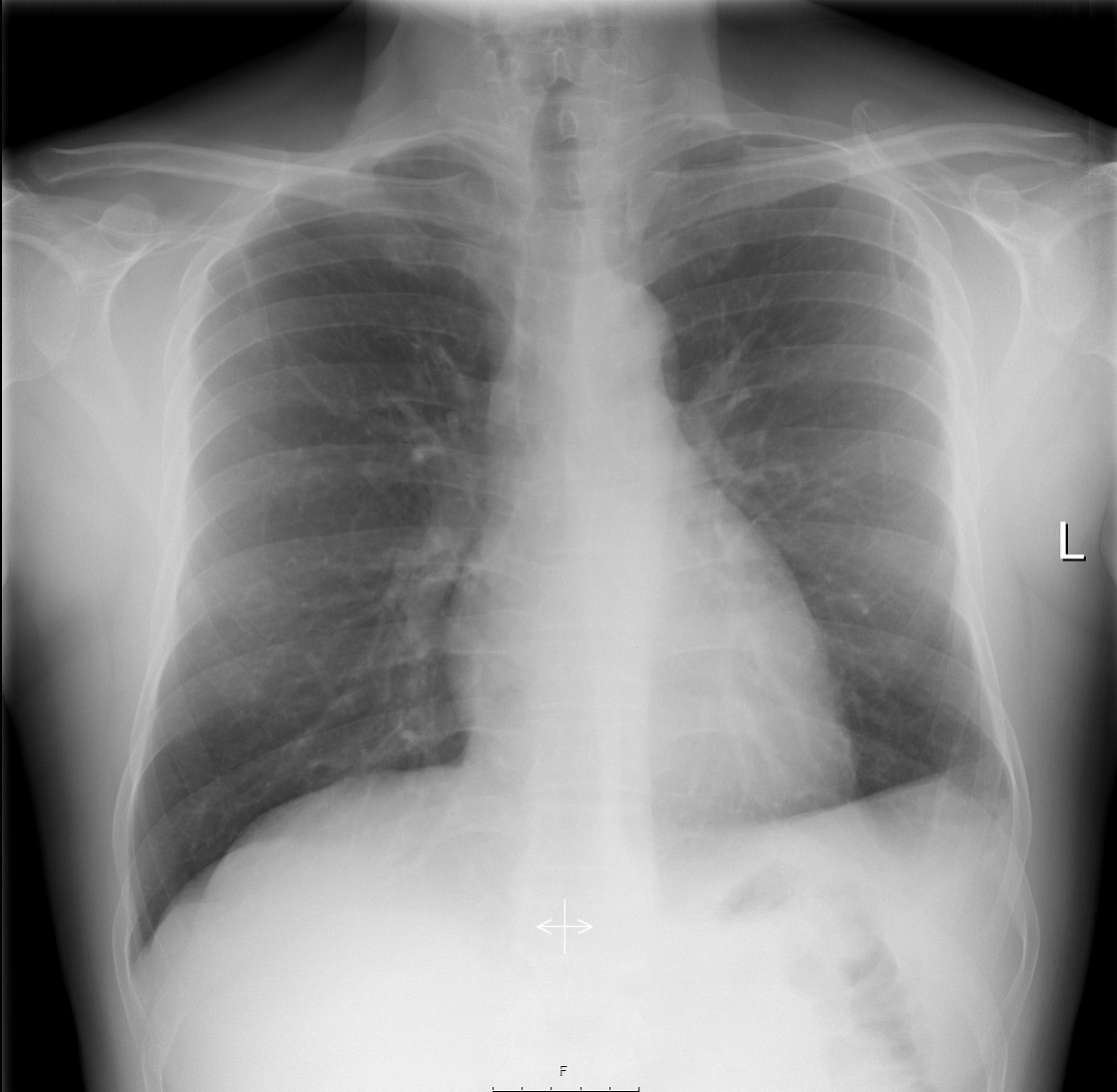
Figure 3 (click to enlarge)
Figure 1. Chest radiograph before drainage and antibiotics
Figure 2. CT thoracic scan before drainage and antibiotics
Figure 3. Chest radiograph after drainage and antibiotics
In the differential diagnosis, a lymphoproliferative process or a tuberculous loculated pleural effusion were considered the main possibilities.
The patient was a daily smoker with no evidence of regular dental check-ups, so poor oral hygiene may have contributed to the condition.
DISCUSSION
F. nucleatum is an immobile, anaerobic Gram-negative bacterium. Lipopolysaccharide endotoxins found in the outer membrane facilitate adhesion and aggregation, allowing tissue invasion and increased virulence. The organism belongs to the Fusobacteriaceae family (13 species), with F. necrophorum and F. nucleatum being the most common pathogens in humans. It is part of the oral commensal flora [1], but can behave as a pathogen in several clinical entities.
The annual incidence of Fusobacterium infections is 0.6–3.5 cases per 1 million population [2]. This micro-organism can cause respiratory, oral, neurological, obstetric and skin infections. In addition, it is linked to colorectal cancer, inflammatory bowel disease and reactivation of latent human immunodeficiency virus-1 infection. It is one of the main causes of empyema. A Bulgarian study with 198 patients, found anaerobic bacteria in 147 (74.2%). F. nucleatum was detected in 27.2% of pleural fluid samples [3], while Dyrhovden et al. reported that of 64 patients with empyema, 37 had an identified micro-organism, including F. nucleatum and/or Streptococcus intermedius [4].
Factors associated with empyema development include bacterial pneumonia, surgery or chest trauma, oesophageal perforation, thoracentesis, subdiaphragmatic infection, spontaneous pneumothorax, bacteraemia, and tobacco or alcohol use [3, 4]. Our patient’s only risk factor was his smoking habit. Diabetes mellitus, renal failure, dialysis, neoplasm and nosocomial infection have been identified as poor prognostic factors [1].
Common clinical manifestations are cough, expectoration, chest pain or fever that can be linked with night sweats, asthenia, anorexia or weight loss. This is the first patient described in the literature who presented only with long-term unexplained weight loss and sweating.
It is important to highlight the difficulty of isolating the micro-organism as it can be hard to obtain valid samples from the lower respiratory tract due to contamination by oral flora. The ideal culture medium is a selective agar called paromomycin-vancomycin Brucella HK. In addition, suboptimal cultivation methods can lead to an underestimation of F. nucleatum frequency [5]. Fusobacterium species are widely susceptible to antibiotics; however, mortality ranges between 4% and 20% depending on the series reviewed and type of Fusobacterium.
In conclusion, empyema due to Fusobacterium can present atypically as unexplained weight loss with night sweats, without fever, cough or chest pain in patients without risk factors or immunosuppression. Antibiotic treatment is usually effective with a good prognosis in most cases.