ABSTRACT
SARS-CoV-2 causes blood hypercoagulability and severe inflammation resulting in an increased risk of thrombosis. Consequently, COVID-19 patients with cardiovascular disease seem to be at higher risk of adverse events. Mondor’s disease is a rare, generally self-limiting, thrombosis of the penis. The pathogenesis of Mondor’s disease is unknown, and it is usually diagnosed through clinical signs and with Doppler ultrasound evaluation. We describe the case of a young man with COVID-19 infection who manifested Mondor’s disease.
LEARNING POINTS
- SARS-CoV-2 infection is associated with an inflammatory response leading to a prothrombotic state and subsequent risk of arterial and venous pathology.
- Superficial vein thrombosis can occur in COVID-19 patients.
KEYWORDS
COVID-19, SARS-CoV-2, vein thrombosis, Mondor’s disease
INTRODUCTION
SARS-CoV-2 infection was declared a pandemic in March 2020 [1]. COVID-19 can cause pneumonia leading to severe respiratory failure requiring intensive care, and also has serious implications for the cardiovascular system [1,2].
Preliminary reports have shown that SARS-CoV-2 causes blood hypercoagulability and severe inflammation, resulting in an increased risk of thrombosis. Consequently, COVID-19 patients with cardiovascular disease seem to be at higher risk of adverse events [3–8].
Mondor’s disease is a rare, generally self-limiting, thrombophlebitis of the superficial veins of the penis (incidence <1.5%) [9–12]. The pathogenesis of Mondor’s disease is unknown, and it is usually diagnosed through clinical signs and with Doppler ultrasound evaluation[9–12]. We describe the case of a young man with COVID-19 infection who manifested Mondor’s disease.
CASE DESCRIPTION
A 28-year-old male patient was admitted to the Emergency Unit complaining pain and had signs of inflammation in the middle third of his penis. The patient reported fever (38.5°C), cough and general distress over the previous 7 or 8 days. His medical history did not show any significant previous disease and he did not have any risk factors for cardiovascular disease. A chest x-ray was negative for pneumonia. Peripheral oxygen saturation (SpO2) was 96% on room air. Blood tests showed haemoglobin 12.3 g/dl, white blood cells 3,460/mm3, platelets 175,000/mm3, C-reactive protein (high-sensibility) 23.20 mg/dl, D-dimer 3.25 g/l and fibrinogen 721 mg/dl. The urine test was normal. Physical examination showed a cord-like induration on the dorsal surface of the penis with locoregional oedema. Ultrasound evaluation revealed thrombosis of the dorsal superficial vein of the penis (Fig. 1). A nasopharyngeal swab for SARS-CoV-2 was taken and was positive. The patient was treated with enoxaparin (4000 IU once a day) and azithromycin for 30 days. After only 48 hours he experienced a significant reduction in pain, and showed complete resolution of all signs of thrombosis 30 days after beginning therapy.
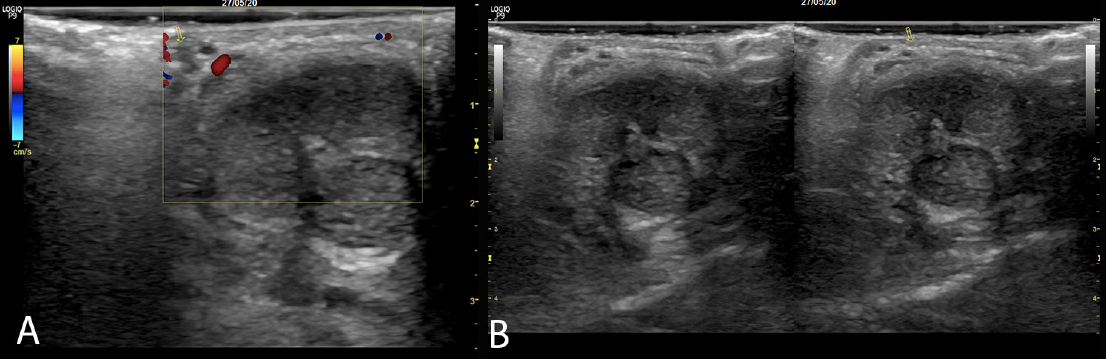
Figure 1 (click to enlarge)
Figure 1 Colour Doppler ultrasound images showing thrombophlebitis of the superficial vein of the penis
DISCUSSION
SARS-CoV-2 infection generally causes a mild disease characterized by fever and cough [1, 2]. However, some 15% of patients develop severe disease requiring hospitalization and oxygen support, and about 5% of these require admission to the intensive care unit [1, 2]. Various data indicate that COVID-19 affects multiple systems including the cardiovascular, respiratory, gastrointestinal, neurological, haematopoietic and immune systems [1–8].
COVID-19 pneumonia induces immunological dysregulation and excessive inflammation, and is characterized by platelet activation, endothelial dysfunction, enhanced thrombin generation and fibrin formation documented by a significant increase in D-dimers leading to consumption of natural coagulation inhibitors [3, 4, 13]. Emerging data reveal that SARS-CoV-2 infection is a risk factor for both arterial and venous thrombosis [4–8]. Several studies have shown that the incidence of symptomatic, objectively confirmed venous thromboembolism (VTE) in COVID-19 patients hospitalized in the ICU can reach 30–40% [8]. An early Chinese study [14] demonstrated that 25% of COVID-19 patients developed lower extremity deep vein thrombosis (DVT) without VTE prophylaxis.
A recent study by Klok et al. described pulmonary embolisms (PE) in 25 of 184 ICU patients with COVID-19 (13.6%), 72% of which were in central, lobar or segmental pulmonary arteries, despite standard dose pharmacological prophylaxis [15-16]. In Italy, Lodigiani et al. showed thromboembolic events (venous and arterial) in 7.7% of patients admitted with COVID-19, corresponding to a cumulative rate of 21% [17]. No data are available on the incidence of superficial vein thrombosis in patients with COVID-19 infection.
Mondor’s disease is a rare pathology with an incidence of 1.39%, and is generally found in patients between 21 and 70 years of age. The aetiology is rarely identified [9–12], but Mondor's disease is associated with several conditions including infection, direct trauma, sexual activity, penis injection, cancer, other vein thrombosis, and a deficit of antithrombin III, Protein C and S [9–12]. There are some reports of surgical thrombectomy, but treatment generally includes anticoagulation with low-molecular-weight heparins and occasionally antibiotics, and treatment of the causal aetiology if identified [9–12].
Our clinical case underlines the fact that SARS-CoV-2 infection is strongly linked to an inflammatory process leading to a prothrombotic state and subsequent risk of arterial and venous pathology. Therefore, in COVID-19 positive patients, the physician must always maintain a high clinical suspicion regarding common and uncommon forms of thrombosis, even in subjects with few risk factors.