ABSTRACT
Blood dyscrasias associated with levetiracetam use can be difficult to identify, especially when other potential differential diagnoses are concurrently present. Here we present a 57-year-old man with metastatic adenocarcinoma of unknown primary origin on levetiracetam who initially presented with an in-stent thrombosis of the right external iliac vein and then developed worsening thrombocytopenia followed by pancytopenia. Levetiracetam was not identified as the culprit until other causes like platelet consumption, heparin-induced thrombocytopenia, idiopathic immune thrombocytopenic purpura, and bone marrow involvement by metastatic disease were ruled out.
LEARNING POINTS
- Levetiracetam can cause both acute and delayed-onset pancytopenia through bone marrow suppression.
- The phenomenon is normally reversible and blood counts improve with drug cessation.
- Clinicians should consider checking a complete blood profile within a month of drug initiation, particularly in high-risk patients.
KEYWORDS
Drug-induced-pancytopenia, thrombocytopenia, levetiracetam, hematology, anti-epileptics
CASE DESCRIPTION
A 57-year-old man with a history of adenocarcinoma of unknown primary origin with metastases to the bone, liver, lungs and brain presented with an acute right lower extremity deep vein in-stent thrombosis. Previously, approximately a year ago, he was found to have high-grade stenosis of the distal right external iliac vein from a large tumour in the right hemipelvis which was stented, and he was started on apixaban. His systemic disease responded well to 11 cycles of carboplatin/paclitaxel and pelvic radiation, but unfortunately, 1 month before the presentation, he developed a right frontal lobe brain metastasis requiring whole brain radiation. He was started on levetiracetam 500 mg and dexamethasone 4 mg twice daily for seizure prophylaxis. His cell counts were within the normal range at the time of initiation of the medication, but on presentation, his platelet count had fallen to 35,000/µl. His white blood cell count (WBC) and haemoglobin were 11,000/µl and 15.1 g/dl, respectively (Table 1. His thrombocytopenia was initially attributed to platelet consumption secondary to the thrombus formation. The peripheral blood smear showed no giant platelets, schistocytes, immature cell lines or platelet clumping. His last cycle of chemotherapy was 2 months prior to presentation. Heparin-induced thrombocytopenia (HIT) was unlikely as his platelet count was low before the initiation of heparin this admission. Haptoglobin, vitamin B12, folate, lactate dehydrogenase, liver function tests and total bilirubin were all normal.
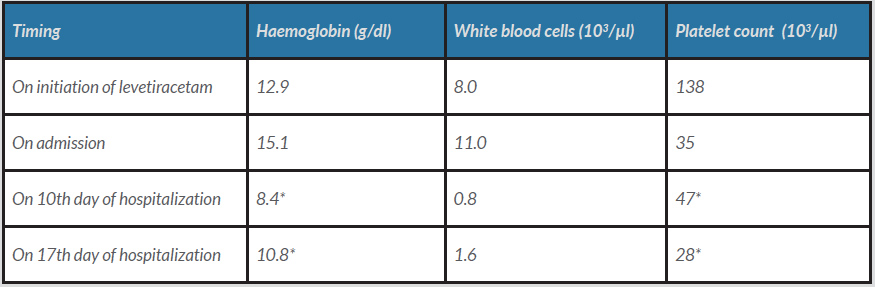
Table 1 (click to enlarge)
Table 1. A summary of the patient’s complete blood picture during the hospital stay (levetiracetam was stopped on the 9th day).
*The patient was receiving transfusions to keep the platelet count above 50,000 µ/l and haemoglobin above 8 g/dl.
Given the thrombocytopenia, he was started on reduced-dose intravenous heparin after mechanical thrombectomy, but his platelet counts continued to drop below the threshold of 50,000/µl despite repeated platelet transfusions. On the 4th day of hospitalization, he developed a left cerebellar bleed due to the progression of brain metastases, requiring heparin reversal with protamine. He underwent a suboccipital craniotomy and levetiracetam was increased to 750 mg twice daily thereafter for seizure prophylaxis following the initial loading dose. All his cell lines continued to drop, and on the 10th day of hospitalization his white blood cell count reached a nadir of 800/µl with an absolute neutrophil count of 700/µl (Table 1). He was also requiring multiple packed red blood cell transfusions to keep his haemoglobin above 8 g/dl. No abnormalities were seen on review of multiple blood smears. Considering metastatic involvement of the marrow, a bone marrow biopsy of the right iliac bone was done which instead revealed a hypocellular marrow (Fig. 1). His pancytopenia was considered secondary to levetiracetam which was switched to topiramate 75 mg twice daily on the 9th day of hospitalization. His WBC gradually improved to 1600/µl on the 17th day of hospitalization, after which he pursued hospice care as his functional status was severely compromised after the cranial surgery.
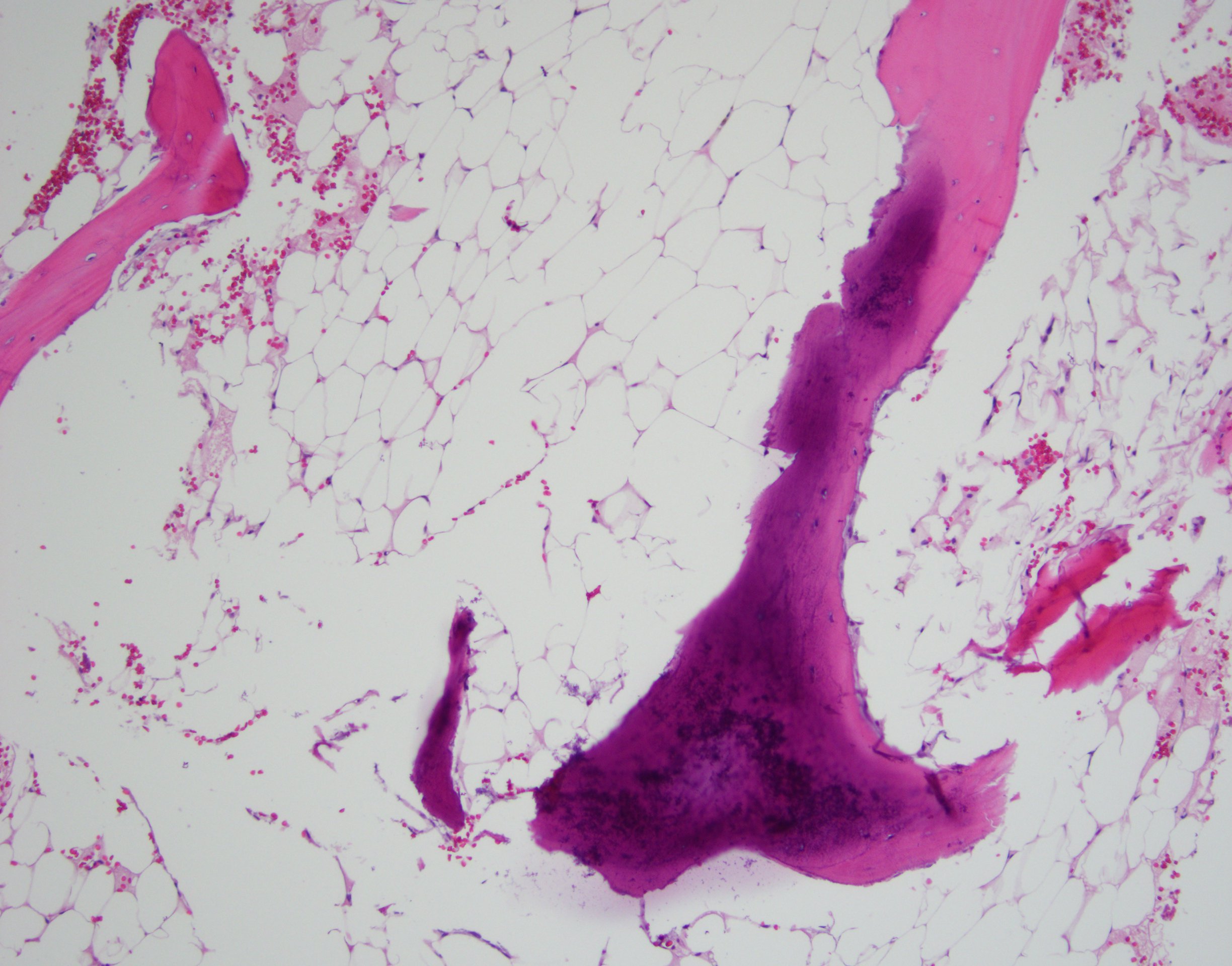
Figure 1 (click to enlarge)
Figure 1. A hypocellular marrow can be seen on the core bone biopsy. No malignant or atypical cells can be visualized (haematoxylin and eosin stain: 10× magnification)
DISCUSSION
Multiple case reports have shown levetiracetam (LEV) to cause both isolated thrombocytopenia and pancytopenia (Table 2) [1–13]. The phenomenon has been seen in both the adult and paediatric populations [1–4]. Usually, the fall in blood counts is drastic and a causal temporal relation with the drug is easy to establish [1,2,5,7]. Consequently, the culprit agent is swiftly identified, and the cessation of use leads to a rapid recovery in counts. In some instances, however, the drop in cell counts can be gradual, and since it is not a common practice to check blood work in patients on LEV, patients can remain on the drug until the blood dyscrasias are incidentally found on laboratory testing for other reasons [8,-10]. It is in such cases, like that of our patient where the thrombocytopenia was noticed a month after starting LEV, that the diagnosis can be challenging. Our patient continued to remain on LEV until the 9th day of hospitalization as his thrombocytopenia was thought to be secondary to platelet consumption following the large venous thrombosis. Despite being on heparin, when his counts continued to fall, other differentials were considered. As he was already on a high dose of steroids, idiopathic thrombocytopenic purpura was unlikely, and there were no abnormalities on review of multiple blood smears. The calculated 4T score resulted in a low probability for HIT. It was only when no metastatic disease was seen on the marrow biopsy that LEV-induced pancytopenia was established as a diagnosis of exclusion. Although similar marrow findings were reported by Oghlakian et al. [8], our patient previously had radiation therapy for his pelvic mass, so whether the histological changes can solely be attributed to LEV is debatable as Mohamed et al. noted a normal cellular marrow in their case of a 6-year-old male [4]. In patients with prolonged exposure, the stability of the haematological profile can be delayed for about a month [8, 9]. Our patient remained transfusion-dependent after drug cessation and then opted for hospice care on day 17. It is unclear what co-morbidities put patients at a higher risk of LEV-related blood dyscrasias, but a large study of 758 patients on LEV identified immunodeficiency as a possible contributor [9], so perhaps a history of metastatic cancer made our patient more vulnerable to this idiosyncratic reaction.
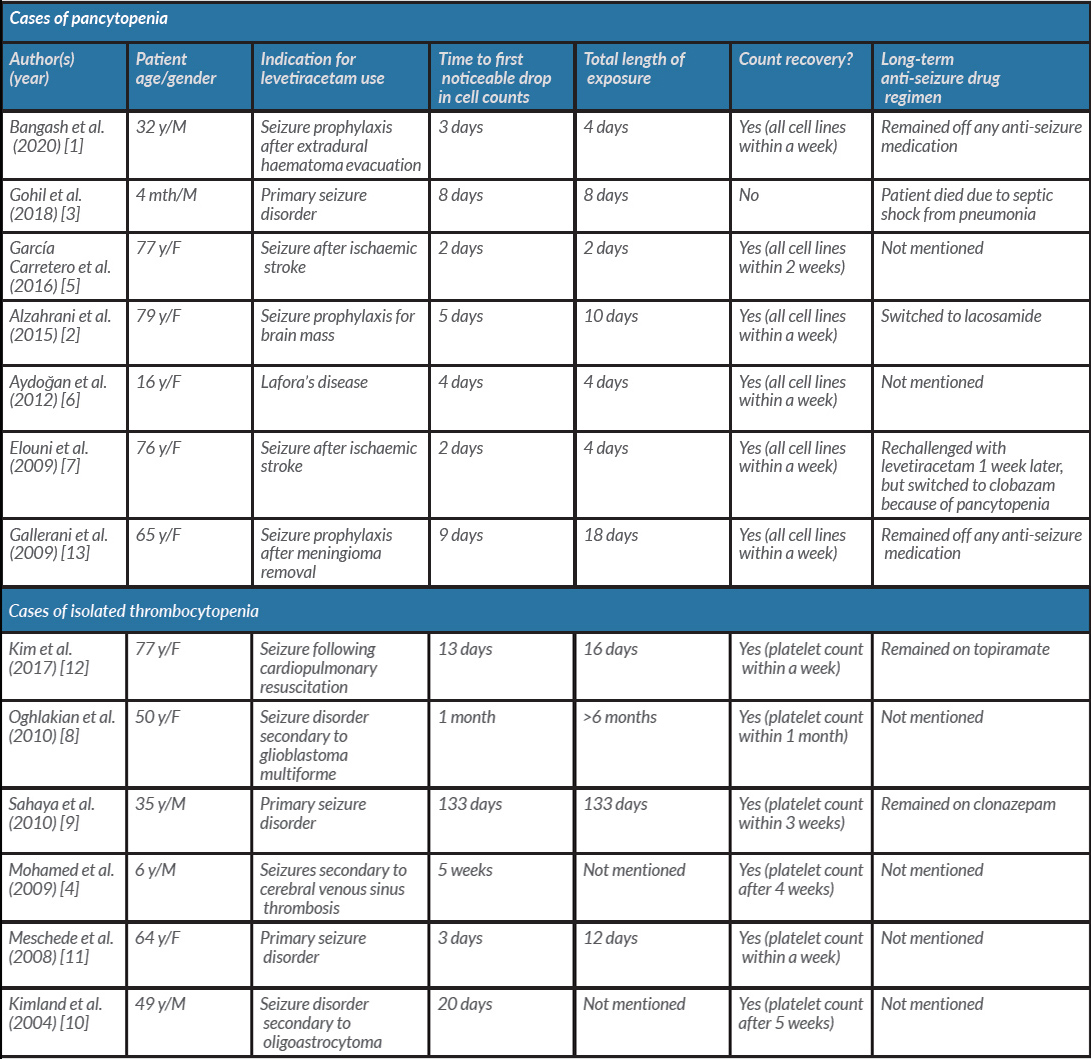
Table 2 (click to enlarge)
Table 2. Summary of previously reported cases of levetiracetam-induced pancytopenia and thrombocytopenia.
F, female; M, male; mth, months; y, years.
CONCLUSION
LEV-induced bone marrow suppression is a rare but important differential to consider in patients with new-onset isolated thrombocytopenia or pancytopenia. It may become difficult to diagnose the condition especially when other differential diagnoses also need to be equally considered. As most cases occur within the first month of initiation of the medication, it may be prudent to check a complete blood count during this time frame and follow patients closely if a drop in cell counts is seen.