ABSTRACT
We present the case of an 84-year-old female patient hospitalized for surgical treatment of a hip fracture who re-tested positive for SARS-CoV-2 with an RT-PCR nasopharyngeal swab approximately 6 months after presenting mild respiratory symptoms with confirmed COVID-19 in April 2020. We discuss the possibility of reinfection, long-term viral shedding and residual positivity, the limitations of RT-PCR swab tests, and the necessity for new testing methods as the COVID-19 pandemic spreads and long-lasting immunity is uncertain.
LEARNING POINTS
- This case suggests that a patient could still test positive on a standard RT-PCR nasopharyngeal swab test for as long as 6 months after previous COVID-19.
- Long-term non-viable viral shedding may be related to the severity of COVID-19 and to persistent pulmonary interstitial damage after COVID-19.
- New testing methods may be required if reinfection becomes common, as testing a patient with known past COVID-19 using a standard RT-PCR swab test could lead to a false positive diagnosis.
KEYWORDS
COVID-19, RT-PCR swab test
CASE DESCRIPTION
An 84-year-old female patient was admitted to our traumatology ward for surgical treatment of a left-side pertrochanteric femoral fracture on 5 October 2020, resulting from a fall-related injury at her nursing home. She was known for diabetes mellitus type 2, coronary, valvular and rhythmic heart disease with stenting of the right coronary artery, aortic valve replacement in 2012 and atrial fibrillation since 2012 currently on apixaban, probable cognitive decline of vascular or mixed aetiology with a history of stroke in 2019, chronic kidney disease and a left hip replacement in 2011. She has lived in a nursing home since November 2019. In early April 2020 she was infected by the novel coronavirus SARS-CoV-2 and tested positive on 9 April 2020 with a RT-PCR nasopharyngeal swab (Table 1). According to the information gathered from the nursing home, she had mild symptoms that did not require hospitalization or extensive medical treatment. Hip repair by osteosynthesis with gamma nailing was performed on 9 October 2020 with no complications due to the delay in treatment caused by the anticoagulation therapy. Two days after surgery, a SARS-CoV-2 RT-PCR nasopharyngeal swab screening test was performed, as standard procedure before transferring the patient back to her nursing home. The RT-PCR test result was once again positive for SARS-CoV-2 (Table 1). The patient did not have any infection or respiratory symptoms during her entire hospital stay, and no other patient or healthcare worker with direct interaction with the patient had shown symptoms or tested positive for SARS-CoV-2. We asked the nursing home for information and no other resident or co-worker had presented any symptoms or tested positive in the last month. The preoperative chest x-rays from 5 October 2020 and 7 October 2020 (Fig. 1, middle and right panels, respectively) showed signs of stable pulmonary interstitial pathology not correlated with symptoms. These findings were compared with a previous chest x-ray from 2019 showing no signs of lung pathology (Fig. 1, left panel).
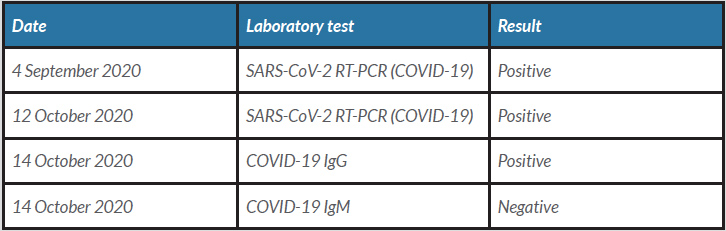
Table 1 (click to enlarge)
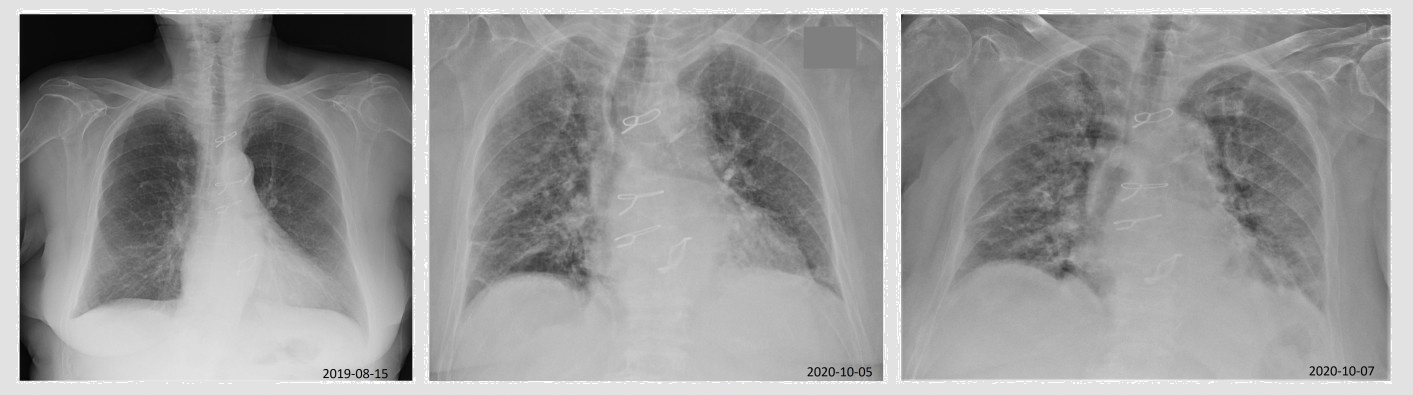
Figure 1 (click to enlarge)
Table 1. Laboratory test results
Figure 1. Chest x-rays from 15 August 2019 (left) before COVID-19 infection and from 5 and 7 October (middle and right), after COVID-19 showing stable interstitial lung damage
DISCUSSION
This case report describes what we believe is the longest known period of positive COVID-19 detection using qualitative RT-PCR nasopharyngeal swabbing after a primary infection [1]. Qualitative RT-PCR diagnosis is based on viral nucleic acid and structural protein detection giving a positive or negative result, but it does not differentiate between the presence of transmissible virus and non-viable viral shedding, and so cannot be correlated with infective viability and active infection [2, 3]. This appears to be a case with long-term positivity after infection, not correlating with disease transmission risk or disease activity [1, 4].
Longer duration of viral shedding and therefore positivity on RT-PCR is thought to be related to disease severity [1]. Our case seems to contradict that premise, as symptoms at the time of primary infection were mild. The chest x-ray performed during hospitalization showed signs of interstitial damage which were not present in a previous chest x-ray from August 2019 and certainly resulted from COVID-19 infection in April [4]. The fact that residual pulmonary abnormalities were present 6 months after infection supports our hypothesis of past SARS-CoV-2 interstitial pneumonia. We believe that these persistent interstitial alterations could also have resulted in long-term non-viable viral shedding and residual RT-PCR test positivity.
The few reported cases of reinfection suggest new infection is possible [5], which however is unlikely in this case as there were no symptoms, no evidence of exposure, and no plausible chain of transmission. The serological test results suggest a post-infection state with the presence of IgG and absence of IgM, which was in agreement with the clinical and chronological information [2, 3]. A positive RT-PCR nasopharyngeal swab a long time (187 days in this case) after the original infection can create a diagnostic dilemma as long-term immunity has not been proven and immunological memory might not be able to protect against new viral mutations [5].
This case report shows the importance of determining good pre-testing probability as well as the limitations of qualitative RT-PCR nasopharyngeal swab testing for screening and diagnosing COVID-19.
In conclusion, a positive RT-PCR swab test in patients with known post-infection status might not be sufficient to determine COVID-19 reinfection, even in the presence of respiratory symptoms, raising concerns as post-COVID-19 status patients become more and more common. A positive RT-PCR swab could also act as a confounder for the diagnosis of other respiratory diseases. If we consider that immunity does not last long, more and more recovered or even vaccinated patients are at risk of reinfection as the COVID-19 pandemic advances. New diagnostic methods might be important in the future to differentiate a new COVID-19 infection from residual viral shedding.