ABSTRACT
Incomplete 90° intestinal rotation in a clockwise direction results in complete common mesentery being placed in a mirror image to and with a similar appearance to complete common mesentery. This rotation places the colon in the right half of the abdominal cavity and the small intestine in the left half of the abdominal cavity.
We report the case of a 19-year-old patient with a history of cerebral palsy secondary to meningitis who presented with melaena and inflammatory anaemia.
CT enterography was performed which showed regular, non-stenosing circumferential wall thickening of the sigmoid colon and rectosigmoid junction compatible with Crohn's disease, which was confirmed by pathophysiology. It also revealed transposition of the colon to the right hemi-abdomen and the small intestine to the left hemi-abdomen, the caecum to the right iliac fossa, and the third portion of the duodenum to the left of the mesenteric vessels.
LEARNING POINTS
- Complete common mesentery in the mirror image is an anomaly of intestinal rotation, placing the colon in the right half of the abdomen and the small intestine in the left half of the abdomen.
- It can be asymptomatic and discovered incidentally during assessment for other conditions.
KEYWORDS
Complete mirrored mesentery, rotation, colon, abdomen, small intestine, Crohn’s disease
INTRODUCTION
Anomalies of intestinal rotation result from the failure of normal embryological rotation and fixation of the primary intestinal loop during embryonic development. The underlying cause of this anomaly is abnormal rotation of the small intestine along the axis of the superior mesenteric artery and can occur at any stage of embryogenesis, involving a part of or the entire intestine [1]. Complete common mesentery in mirror image suggests a type of incomplete rotation where the intestine is rotated 90° clockwise, but has a similar appearance to complete common mesentery [2]. Intestinal malrotation in adults may be associated with irritable bowel syndrome or related minor abdominal symptoms [3]. We report a rare case of the mirrored appearance of complete common mesentery associated with Crohn's disease diagnosed in adulthood.
CASE DESCRIPTION
A 19-year-old man followed for cerebral palsy secondary to meningitis, presented with melaena and a well-tolerated anaemic syndrome. On physical examination, he was conscious and haemodynamically stable. His temperature was 37.1°C, respiratory rate was 16 breaths per minute, pulse was 92 beats per minute, and blood pressure was 110/70 mmHg. Blood tests revealed inflammatory anaemia with haemoglobin of 8 g/dl and a drop in haematocrit. C-reactive protein (CRP) was increased to 102.4 mg/l. The rest of the examination was unremarkable.
The patient was referred to the radiology department for CT enterography, which revealed circumferential, regular and non-stenosing wall thickening of the sigmoid colon and the rectosigmoid junction measuring 14 mm at maximum thickness (Fig. 1). The scan also revealed the presence of the entire colon in the right side of the abdominal cavity pushing the liver forward on the contralateral side, and the small intestine located on the left (Fig. 2). The duodenum was located anterior to the mesenteric vessels, while the caecum was in the right iliac fossa (Fig. 3). The superior mesenteric vein was located in front of its twin artery (Fig. 4). The rest of the organs were in their normal position.

Figure 1 (click to enlarge)
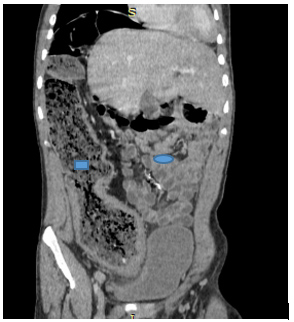
Figure 2 (click to enlarge)
Figure 1. Abdominal CT scan with contrast in the axial plane showing circumferential, regular and non-stenosing thickening of the wall of the sigmoid colon (blue star)
Figure 2. Abdominal CT scan with contrast in the coronal plane showing the large bowel (blue box) in the right side of the abdomen and the small intestine (blue oval) in the left side of the abdomen
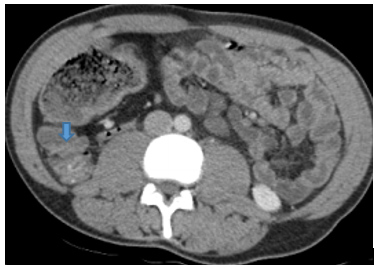
Figure 3 (click to enlarge)

Figure 4 (click to enlarge)
Figure 3. Abdominal CT scan with contrast in the axial plane showing the caecum in the right iliac fossa (blue arrow)
Figure 4. Abdominal CT scan with contrast showing the superior mesenteric vein anterior to the artery (blue arrowhead)
DISCUSSION
Malrotation of the midgut in adults is rare with a reported incidence of 0.0001–0.19% in adults [3]. The true incidence in adulthood is difficult to estimate because patients remain asymptomatic. Knowledge of the embryology of bowel rotation is key to understanding these abnormalities.
During embryological development, the intestine undergoes complex phenomena of reintegration, rotation and apposition [4,5]. Embryologically, the first rotation takes place before the tenth week of gestation when the primary intestine is still located outside the abdomen. This rotation places the previteline (small intestine) portion on the right and the postviteline (colon) portion on the left. If rotation ceases at this point, complete common mesentery results [1, 6].
Complete common mesentery results if intestinal rotation stops at 90°. Thus, the colonic frame is located on the left and the small intestine on the right, the caecum in an anterior and middle position, and the superior mesenteric artery on the right of the superior mesenteric vein[6].
We describe a case of incomplete 90° rotation leading to an arrangement similar to complete common mesentery but with rotation in the clockwise direction, resulting in a mirror image of complete common mesentery [2].
This abnormality of rotation of the mesentery brings the colonic frame into the right half-abdomen and the small intestine into the left half-abdomen, with the caecum in its normal position at the level of the right iliac fossa. The third portion of the duodenum is in front of the mesenteric vessels. This intestinal malrotation remains asymptomatic and is therefore frequently not diagnosed until adulthood [3, 4]. The complete common mesentery is often discovered either incidentally or as part of investigation of a tumour or inflammatory pathology of the digestive tract [4].
Likewise, the condition in our patient was also found incidentally during investigations for Crohn's disease and confirmed by colonoscopy with biopsy and pathophysiology of the biopsy specimen. Intestinal malrotation is often an incidental finding and generally does not require surgical intervention [3]. Our patient was started on infliximab 5 mg/kg according to the protocol for Crohn's disease. The evolution was favourable.
CONCLUSION
Mirror appearance of the complete common mesentery results from incomplete rotation similar to that causing complete common mesentery but in a clockwise direction. It results in positioning of the entire colon to the right and the small intestine to the left in the abdominal cavity. This intestinal rotation abnormality remains asymptomatic, and is often discovered incidentally in adulthood during investigations carried out for other purposes.