ABSTRACT
Introduction: Venous air embolism is rarely seen, can be fatal and is associated mostly with large central venous catheters and mechanical ventilation. Some cases due to peripheral intravenous access have also been reported.
Case Description: We present a case of intracranial venous air embolism most likely secondary to peripheral cannulation. On admission, the patient was drowsy with a suddenly deteriorating Glasgow coma scale score. This case emphasizes cautious cannula insertion and close monitoring of the patient in the event of complications.
Conclusion: Intravenous cannulation is common but care should be taken to avoid catastrophic complications. Consider air embolism as the differential diagnosis if a patient has a low level of consciousness after an intravenous cannula is inserted.
LEARNING POINTS
- A reduced level of consciousness in a patient should be quickly recognised and the differential diagnosis of air embolism considered.
- Peripheral vascular cannulation should be carefully monitored.
- High-flow oxygen and efficient monitoring of the patient are required.
KEYWORDS
Air embolism, intravenous, peripheral cannulation, iatrogenic
CASE DESCRIPTION
A 71-year-old male care home resident attended the emergency department with drowsiness and difficulty breathing.
Initial assessment revealed that his airway was patent, respiratory rate was 24, widespread wheeze was heard all over his chest, blood pressure was 76/40 mmHg and heart rate was 115. His Glasgow coma scale score was 11/15. After resuscitation, his blood pressure increased but he remained drowsy. The care home staff advised that he had chronic obstructive pulmonary disease and had been short of breath more than usual. He was treated with intravenous hydrocortisone, co-amoxiclav and gentamicin on the grounds of sepsis secondary to a chest infection. His arterial blood gas analysis showed type 2 respiratory failure and ECG showed sinus tachycardia.
His Glasgow coma scale score worsened and he became drowsier. Computed tomography of the head showed multiple foci of bilateral surgical emphysema (Figs. 1 and 2). Given the distribution of this gas, some of which was seen within the cavernous sinus, the right internal jugular vein, both ophthalmic veins as well as a serpiginous, likely vascular structure within the spinal canal, it was likely related to intravenous cannulation with two large-bore 18G and 20G cannulas. No other possible causes were identified and there was no history of trauma. The patient was cautiously given oxygen which resulted in a slow but complete recovery of consciousness.
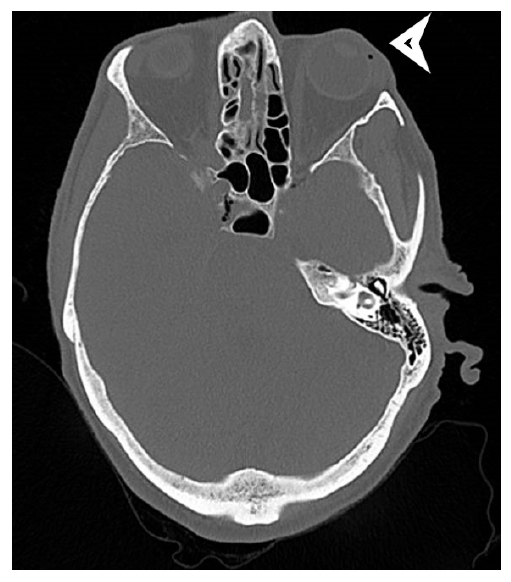
Figure 1 (click to enlarge)

Figure 2 (click to enlarge)
Figure 1. Computed tomography (axial view) of the brain showing air embolism in the superior ophthalmic vein
Figure 2. Computed tomography (axial view) of the brain showing widespread air locules
DISCUSSION
Air embolism is caused by the direct introduction of air via surgical procedures including craniotomy, laparoscopic procedures and caesarean section [1]. Air embolism acquired by the vascular route requires an iatrogenic air bubble to convert into an embolus [2]. The main causes include the insertion or removal of a central venous catheter [3, 4].
This case was remarkable for the insertion of wide-bore cannulas and suddenly reduced consciousness. There was nothing in the patient's history to suggest that this could have been caused by any other aetiology. The patient was very slow to recover. His level of consciousness remained low but he was treated with oxygen and gradually improved. When he regained full consciousness, a complete neurological examination was performed which revealed normal gaze, no visual disturbance, no limb weakness and no facial weakness. A mild tremor was noted but was of no significance. There was no sensory loss and no aphasia, but slow speech and mild slurring of some words were noted. No abnormalities were detected in extinction and inattention. A repeat computed tomography of the head showed complete resolution of air embolism.
Peripheral intravenous treatment is usually given for a short period of time (2–5 days) and is mainly used to administer intravenous fluids, drugs, blood and blood products and also for nutritional support in the form of TPN. Ideally treatment via alternative routes should be administered where possible to reduce cannulation-related risks such as infection and the introduction of an air embolism. However, the intravenous route is necessary when a patient is not taking anything orally or immediate intervention with rapid bioavailability is required. Peripheral venous catheters are relatively easy to insert and are comfortable for the patient. The first step should be to stop using the cannula to avoid worsening the air embolism. The main treatment is high-flow oxygen which will help reduce the size of the embolism [5]. Swift recognition of venous air embolism is crucial, as a missed diagnosis can result in irreversible damage. Venous air embolism should be considered in patients with findings similar to those in this case.