ABSTRACT
Acute intoxication with 2,4-D dimethylamine is rare, often fatal and can cause signs and symptoms in different organ systems. This case report describes the effectiveness of alkaline diuresis as a life-saving treatment for chlorophenoxy intoxication, especially in healthcare facilities without access to haemodialysis. A patient had attempted suicide by ingesting 2,4-D dimethylamine, with toxic effects on the central and peripheral nervous systems, and the gastrointestinal and respiratory systems. However, she significantly improved after alkaline diuresis, accompanied by resuscitation, decontamination of the gastrointestinal system, and supportive therapies.
LEARNING POINTS
- With no known of antidote, 2,4-D dimethylamine intoxication can be fatal if not treated promptly.
- Alkaline diuresis can be a life-saving treatment, especially in rural area with no access to haemodialysis.
- Treatment with alkaline diuresis can give a good result in patients who present with severe intoxication.
KEYWORDS
Herbicide intoxication, 2,4-D dimethylamine, alkaline diuresis, chlorophenoxy
INTRODUCTION
The use of 2,4-D dimethylamine is becoming more common due to increasing resistance to the herbicides glyphosate and paraquat [1]. Therefore, growth in the number of cases of 2,4-D dimethylamine intoxication should be anticipated. This herbicide shows a variety of dose-dependent toxicity mechanisms, including cell membrane damage, uncoupling of oxidative phosphorylation, and disruption of acetyl coenzyme A metabolism [2]. Toxic effects may involve the nervous system, heart, lungs, liver, kidney, muscles and endocrine system [3]. In many cases, the results are fatal [2, 4]. This report describes the effectiveness of alkaline diuresis as a life-saving treatment for 2,4-D dimethylamine intoxication with severe symptoms in a rural area.
CASE DESCRIPTIONS
A 19-year-old woman attended the public health centre with vomiting, abdominal pain, malaise, and a burning sensation in her chest. She had deliberately drunk 65 ml of DMA 6 solution containing the active ingredient 2,4-D dimethylamine 825 g/l. She was fully conscious and received normal saline and activated charcoal. However, 15 minutes later, she rapidly lost consciousness and was immediately referred to hospital.
On admission, she presented with a Glasgow Coma Scale of E2M4V2. Blood pressure was 100/70 mmHg, pulse 105 beats per minute, respiratory rate 32–36 times per minute, temperature 37.5°C, and oxygen saturation 96–98% with oxygenation 4 litres per minute. Muscle tone was decreased and tendon reflexes were absent. Routine blood tests showed leucocytosis with absolute neutrophilia. Blood gas analysis revealed partially compensated respiratory alkalosis, while routine urine examination revealed haematuria. The patient was diagnosed with herbicide intoxication with loss of consciousness, sepsis and septic shock, stress ulcers, transaminitis, and attempted suicide. She was treated in the intensive care unit with oxygenation, intravenous fluids with normal saline, cefotaxime, omeprazole and ondansetron. Gastric lavage was performed. Initially, the liquid was blackish-brown in colour, but after the administration of 200 ml of fluid, the liquid became clear. Antacids and sucralfate were given to treat stress ulcers.
Over the next 7 hours, the patient’s condition deteriorated. She became unresponsive to painful stimuli, her blood pressure decreased to 80/50 mmHg, and blood clots were found in the nasogastric tube. Fluid resuscitation was given immediately with 1500 ml normal saline, but blood pressure did not reach the target. The patient was given a vasopressor and reached the systole target pressure of >100 mmHg. Omeprazole was given in a loading dose, then continued with maintenance infusion. Tranexamic acid was also given.
By the second day, the patient’s temperature had reached 38.6°C and paracetamol was given. Alkaline diuresis was initiated by giving 1 mEq/kg sodium bicarbonate in 0.9% normal saline 100 ml intravenously within 30 minutes, and then supplemented with 75 mEq of sodium bicarbonate and 25 mEq of potassium in 500 ml of 5% dextrose within 8 hours. Furosemide 20 mg was given every 12 hours intravenously for 8 days, with gradual dose reduction starting from the fifth day. Furosemide was then continued orally. Intravenous dexamethasone is also given to treat cerebral oedema.
On the fourth day, the patient’s leukocyte count began to decrease, but liver enzyme levels were increased. She started responding to treatment and became fully conscious after 5 days and began accepting oral therapy. She was transferred to a regular ward on the tenth day and discharged on the twelfth day in a stable condition (Fig. 1).
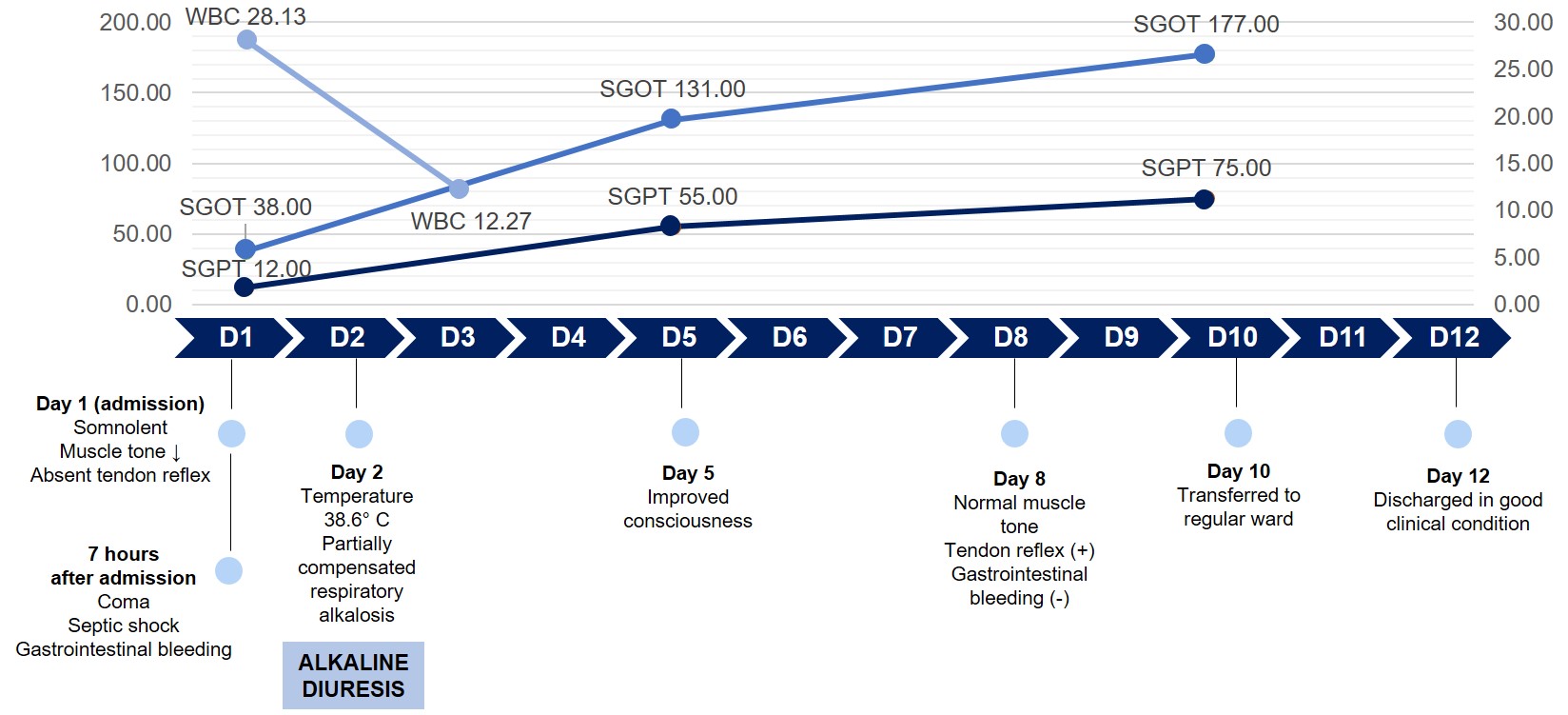
Figure 1 (click to enlarge)
Figure 1. Timeline of clinical condition
DISCUSSION
The patient was diagnosed immediately based on her history; early identification of the causative agent early is very useful in management. The amount of herbicide consumed was quite large (65 ml) since this was an attempt at suicide. In this case, a toxic effect was seen in multiple organ systems, including the gastrointestinal, respiratory and nervous systems. Septic shock was also found as demonstrated by symptoms, physical examination and laboratory results.
Until now, there has been no specific antidote for 2,4-D dimethylamine intoxication. Chlorophenoxy is a weak acid (pKa 2.6 for 2,4-D) that is excreted in the urine in the same form. Intravenous sodium bicarbonate acts by increasing urine pH. Renal excretion is better in alkaline urine conditions (63 ml/min at pH 8.3) than in acidic conditions (0.14 ml/min at pH 5.1) [2]. For each unit increase in urine pH, the clearance of 2,4-D by the kidney is estimated to increase nearly five-fold [3]. Therefore, the administration of sodium bicarbonate with a target urine flow of 4–6 ml/minute will increase the excretion of 2,4-D dimethylamine. In this case, urine pH after alkaline diuresis was not evaluated, so the renal clearance and half time of 2,4-D in this patient could not be determined. According to the literature, hypokalaemia may occur during alkaline diuresis and so sodium bicarbonate should be accompanied by potassium administration [2].
Haemodialysis is more efficient than alkaline diuresis and can induce the release of toxic substances without manipulating urine pH and the requirement for large amounts of intravenous fluids. However, the treatment plan adopted is ultimately based on the availability of facilities. In addition to haemodialysis, there are case reports describing plasmapheresis as a therapy for intoxication, but there is limited evidence to support this approach in the treatment of severe 2,4-D dimethylamine intoxication [3, 4].
In cases of mild intoxication, supportive therapy might be sufficient, but, in cases of severe intoxication, treatment with alkaline diuresis or haemodialysis is required [4]. However, there is no severity classification as a reference to determine the most appropriate therapy.
Shock and loss of consciousness in cases of 2,4-D dimethylamine intoxication indicate a poor prognosis. However, timely administration of an alkaline diuresis can be life-saving. Recovery can be achieved in weeks to months despite initial severe toxicity [2, 4].
CONCLUSIONS
2,4-D dimethylamine intoxication is rare, does not have an antidote, and has high morbidity and mortality. Alkaline diuresis as a life-saving treatment must be accompanied by other therapies including initial emergency resuscitation, decontamination of the gastrointestinal system, and supportive treatment.