ABSTRACT
Hydropneumopericardium is a rare event with a risk of serious complications. Timely diagnosis and treatment is important as it can improve prognosis. We report the case of a 77-year-old male patient who presented with acute interscapular pain which developed during a meal. An oesophago-pericardial fistula was found in the context of malignant oesophageal disease.
LEARNING POINTS
- Hydropneumopericardium secondary to oesophageal tumour is a rare but life-threatening finding that has a very poor prognosis.
- A high level of suspicion is needed, as the clinical manifestations are very unspecific and timely treatment can improve prognosis.
- Successful management of an oesophago-pericardial fistula includes surgical treatment and antibiotic therapy.
KEYWORDS
Hydropneumopericardium, oesophageal tumour, oesophago-pericardial fistula
CASE DESCRIPTION
We present the case of a 77-year-old man diagnosed 10 months earlier with epidermoid carcinoma of the middle oesophagus presenting with involvement of the left main bronchus and descending thoracic aorta. He was later diagnosed with brain metastases and because of aphagia, an oesophageal prosthesis was inserted.
He was admitted to the emergency department because of a sudden interscapular pain which developed during a meal, with shoulder irradiation but no other associated symptomatology.
On admission, the patient was hypotensive, with no differential blood pressure between the limbs and with arrhythmic heart sounds. He had hyperlactacidaemia (lactic acid 4.0 mmol/l, normal: <2.0 mmol/l) and new onset atrial flutter. The biochemical work-up was unremarkable for inflammatory parameters. No elevation in cardiac biomarkers was found. Due to suspicion of aortic dissection, he underwent thoracic computed tomographic angiography (Fig. 1) that revealed the presence of air and fluid in the pericardial space (hydropneumopericardium) due to oesophageal perforation because of tumour invasion.
Due to the documented disseminated malignancy and poor patient status, priority was given to comfort measures and the patient died within 24 hours.
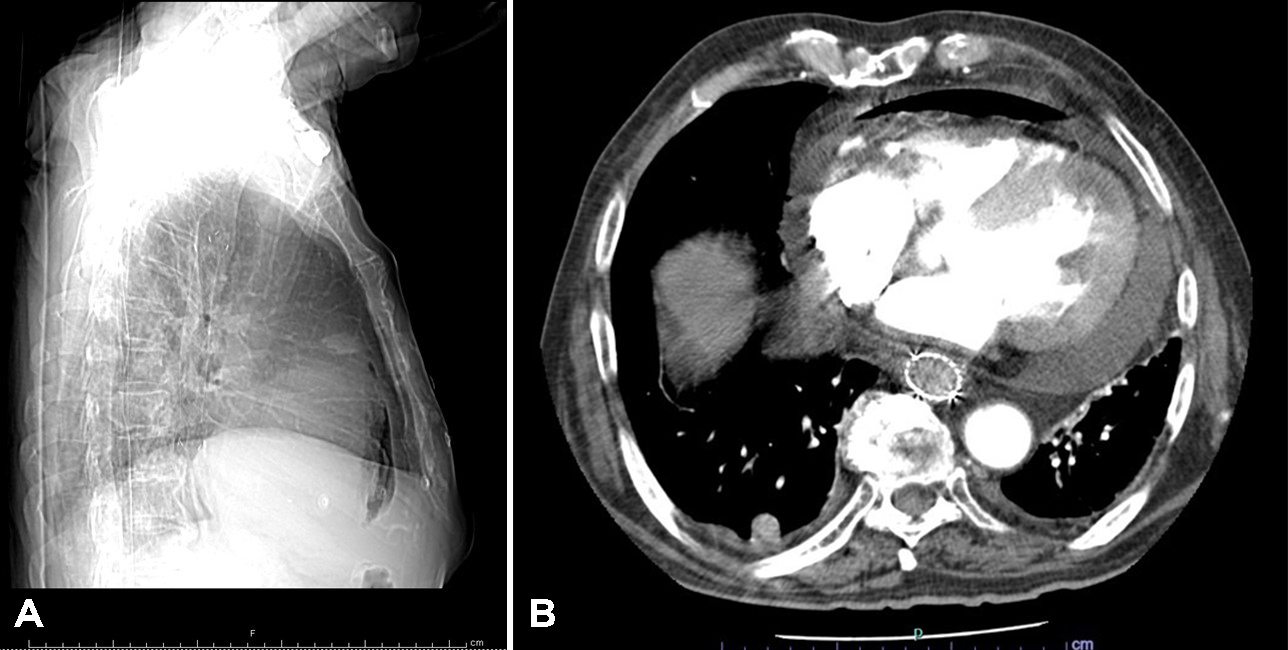
Figure 1 (click to enlarge)
Figure 1. Computed tomographic topogram (A) and computed tomographic scan of the chest with contrast (B) showing the presence of air and a fluid component (indicated by a blue arrow) in the pericardial space
DISCUSSION
Pneumopericardium is a rare event that can occur in the context of trauma, pericardial infection, and fistulization from adjacent structures, or secondary to procedures such as pericardiectomy [1, 2].
Oesophago-pericardial fistula is an uncommon but life-threatening finding whose aetiology includes some benign conditions but also trauma and malignant oesophageal disease. The subsequent infection that spreads to the pericardium is usually devastating, with a high mortality rate [3].
Hydropneumopericardium secondary to oesophageal tumour is a very rare complication and has an extremely poor prognosis, which can be explained by the worsening of the patient’s general condition, late diagnosis and progression to mediastinitis and severe sepsis. Therefore, a high level of suspicion is needed to make a diagnosis, as the clinical manifestations can be very unspecific and timely treatment can improve prognosis [2, 3]. Physical examination plays a crucial role in haemodynamic assessment, stratification of clinical severity, and assessment of the need for emergency intervention, complemented by imaging studies.
Successful management of an oesophago-pericardial fistula should include pericardial drainage, surgical closure of the fistula and antibiotic therapy, which was not possible in the case reported here due to the extent of the oesophageal malignancy and poor patient status [2, 3].
The authors emphasize that, despite being a rare event, hydropneumopericardium should be considered in the differential diagnosis of patients who present with acute chest pain, especially in the presence of neoplasms involving the cardiothoracic or gastric region.