ABSTRACT
Obesity has become a major public health problem with increased prevalence and is associated with cardiovascular mortality. Phentermine is approved for short-term obesity treatment in conjunction with lifestyle modifications. Palpitations are a well-documented side effect of phentermine, but atrial fibrillation (AF) is rarely reported. We present a case of new-onset AF in a healthy woman who had been recently started on phentermine for weight loss.
LEARNING POINTS
- Atrial fibrillation usually occurs secondary to intrinsic disorders such as hypertension, coronary artery disease, abnormal heart valves, thyroid dysfunction and medication side effects.
- Phentermine is used for a short period together with diet and exercise to treat obesity; atrial fibrillation is an unusual cardiovascular side effect of phentermine that warrants clinician caution.
- The importance of medication reconciliation is exemplified in this case as it is essential to rule out secondary causes of atrial fibrillation, including medication side effects.
KEYWORDS
Phentermine, obesity, atrial fibrillation
INTRODUCTION
Obesity is a significant risk factor that is strongly associated with cardiovascular complications. In addition to diet and exercise, pharmacotherapy remains a popular option for treating obesity, with phentermine being the most commonly used drug. Phentermine (Adipex), a centrally acting appetite-suppressant and norepinephrine stimulant, is an adjunctive drug primarily prescribed for obesity (BMI >30) refractory to 3–6 months of lifestyle modification [1]. Short-term use is recommended because of the relative increase in sympathetic tone and adverse effects such as insomnia, dry mouth, dizziness, hypertension and tachycardia. This case report explores AF as a potentially severe adverse outcome of phentermine in an obese but otherwise healthy female.
CASE DESCRIPTION
A 49-year-old obese woman with no significant medical history except for migraines, presented with acute onset of dizziness and palpitations. The patient stated that she works as a teacher and was in her class when she felt like the room was spinning around her and her heart was racing. She denied any chest pain, shortness of breath, passing out, or any other symptoms. She had not experienced any similar episodes in the past. She had been started recently on phentermine 37.5 mg for weight loss by her primary care physician (PCP); her other medication was Excedrin (aspirin/paracetamol/caffeine) for migraines. Vital signs were a blood pressure of 132/86 mmHg, heart rate of 156 beats/minutes, respiratory rate of 18 breaths/min, temperature of 37°C, and oxygen saturation of 99% on room air. Cardiovascular examination revealed irregular tachycardia, with normal S1 and S2, and no murmurs. The rest of the physical examination was within normal limits. A twelve-lead electrocardiogram (EKG) revealed narrow complex tachycardia, with irregular rhythm consistent with a diagnosis of AF with a rapid ventricular response (Fig. 1). A complete blood count, basic metabolic panel and thyroid panel were within normal ranges. A urine drug screen was negative. A transthoracic echocardiogram (TTE) showed a normal ejection fraction of 60–65%, no regional wall motion abnormalities, and normal atrial and ventricular sizes. The patient was started on a diltiazem drip for rate control, later titrated to oral diltiazem 30 mg every 6 hours. She achieved rhythm control with an amiodarone drip and was anticoagulated with heparin. Her heart rhythm converted to a sinus rhythm with a regular heart rate of 80–90 beats/minute. The patient’s CHA2DS2-VASc score for AF stroke risk was 1, so she was started on aspirin 81 mg daily. She remained stable and was discharged on aspirin 81 mg and metoprolol 25 mg. She was advised to discontinue phentermine and to follow up with her PCP within 1 week.
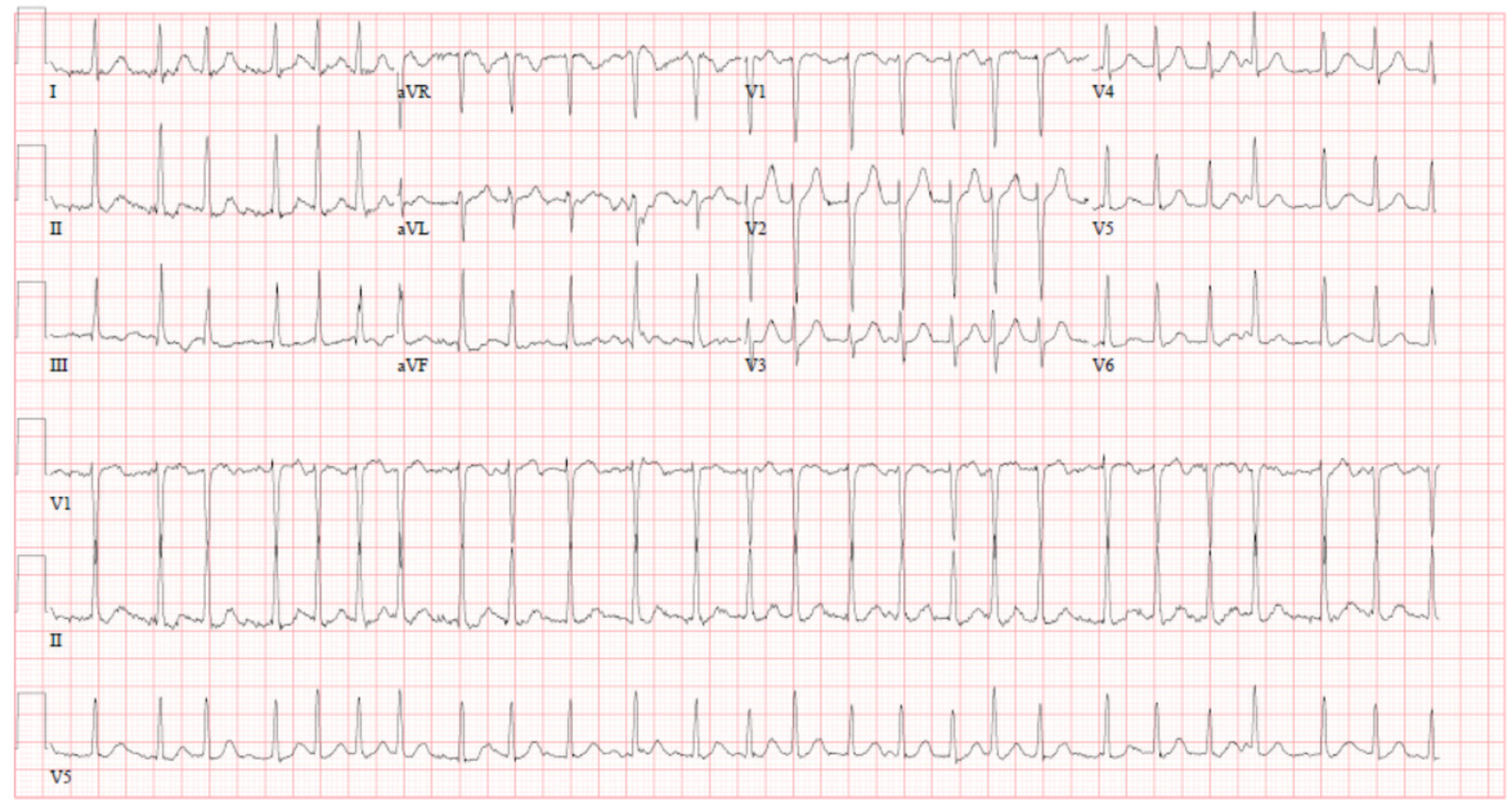
Figure 1 (click to enlarge)
Figure 1. Atrial fibrillation with a rapid ventricular response and a heart rate of 156 beats/minute
DISCUSSION
Phentermine is a prescription medication for weight loss. It is a sympathomimetic stimulant that is chemically similar to amphetamine. It suppresses the appetite by norepinephrine release in the hypothalamus, reducing hunger perception and stimulating peripheral epinephrine and norepinephrine release, causing fat cells to break down their stored fat [1].
Common phentermine side effects include nausea, vomiting, diarrhoea, constipation, dry mouth, restlessness, nervousness, headaches, tremors and insomnia. It has a very small risk of addiction. The main cardiovascular adverse effects are palpitations, mild tachycardia and elevated blood pressure [2]. Cardiovascular contraindications for the use of phentermine are a history of coronary artery disease, stroke, arrhythmias, congestive heart failure and uncontrolled hypertension [3]. AF has not been a well described adverse effect of phentermine. To our knowledge, phentermine-induced AF has been reported only twice in the literature.
In 2012, a 43-year-old man who had severe obesity and obstructive sleep apnoea (OSA) was started on a high-protein diet and phentermine. He developed AF 3 weeks later and required cardioversion during his hospital stay. Apovian et al. concluded that his history of OSA complicating right-sided heart failure and starting phentermine were the triggers for AF [4].
In 2015, a case of phentermine-induced AF with resulting cardiomyopathy was reported in a 65-year-old man who had AF with a rapid ventricular response to 180 beats/minute. He had been on phentermine for 3 years with up to five doses weekly which was the likely precipitant of his AF-induced cardiomyopathy as work-up was negative and other obvious causes were ruled out [5].
Our patient was on Excedrin which contains caffeine. It is unclear if caffeine might have potentially exerted an additive synergistic effect with phentermine to generate arrhythmia. Our case emphasizes the importance of a thorough history and physical examination that can provide clues to an underlying diagnosis.