ABSTRACT
Inhalants are common drugs of abuse. Hydrocarbons, the active ingredient in most inhalants, exert depressant effects on the central nervous system, causing a ‘high’. In the heart, hydrocarbon toxicity can predispose patients to arrhythmias and heart failure through increased sympathetic susceptibility. We present the case of a 28-year-old female who developed dilated cardiomyopathy in the setting of chronic inhalant abuse.
LEARNING POINTS
- Chronic inhalant abuse can lead to cardiac arrhythmia and heart failure.
- Chronic inhalant abusers should be screened for signs of heart failure.
- Severe hydrocarbon toxicity can cause sudden sniffing death syndrome.
KEYWORDS
Inhalant, cardiomyopathy, hydrocarbon toxicity
INTRODUCTION
Inhalants are substances that are grouped by a common route of use as opposed to a similar mechanism of action [1]. Inhalant use is most common among teenagers, but can continue into adulthood. Prevalence of lifetime inhalant use among 12th graders in the United States was 11.1% in 2006[1]. Hydrocarbons are used as solvents in inhalants and have several physiologic effects [2]. They exert depressant effects on the central nervous system, causing the ‘high’ most abusers chase. In severe cases of toxicity, death can result from cardiac arrhythmia, known as sudden sniffing death syndrome [1]. We present the case of a 28-year-old female who developed acute dilated cardiomyopathy as a result of inhalant use.
CASE DESCRIPTION
An electrocardiogram was performed and showed sinus tachycardia with a QTc interval of 500 ms. Brain natriuretic peptide was elevated at 513 pg/mL. A computed tomography (CT) angiogram of the chest was performed and pulmonary embolism ruled out. However, parenchymal infiltrates and large right and left pleural effusions were noted. The patient, known to us from an admission 4 years earlier, had CT scans available for comparison that also showed bilateral pleural effusions. However, her current effusions were worse. Additionally, the patient had a lung biopsy during her prior admission that looked for cryptogenic organizing pneumonia, which was negative. On this occasion, she was started on antibiotics for a possible infectious cause and admitted for management of the pleural effusions. A pulmonary consult recommended ruling out infectious causes, bronchoscopy with biopsy, chest tube placement, and echocardiogram.
Acid-fast bacilli smears and cultures were negative for tuberculosis, as was a Mycobacterium tuberculosis/rifampin polymerase chain reaction (PCR). HIV testing was negative as well. The patient’s chest tube drained 3.6 L in the first 24 hours. Pleural fluid analysis showed exudative effusion with lymphocytic predominance with the presence of reactive mesothelial cells. Serum protein electrophoresis was obtained, which showed paraproteinemia. A repeat lung biopsy was negative for malignancy and the pulmonary team believed her lung findings were due to chronic inhalational injury.
An echocardiogram showed beat-to-beat variation in the left ventricular outflow, known as pulsus alternans (Fig. 1). This is suggestive of low cardiac output. There was severe global hypokinesis of the left ventricle, with normal right ventricular function. Left ventricular ejection fraction was 25%, a decrease from 50% on the echocardiogram from her previous admission. A nuclear stress test was significant for a small, moderately severe inferolateral wall defect that appeared worse on rest than post-stress, which likely represented an artifact. The patient was deemed to be at high risk for ventricular arrhythmia and a LifeVest personal defibrillator was arranged. She was discharged from the hospital on diuretics, but did not return for an outpatient repeat echocardiogram.
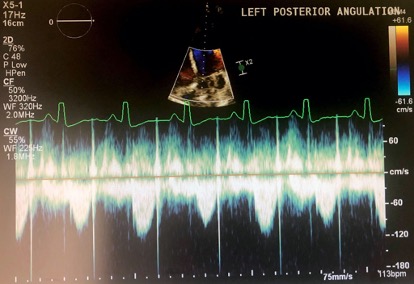
Figure 1 (click to enlarge)
Figure 1. Echocardiogram showing pulsus alternans
DISCUSSION
There are different ways to use inhalants, such as sniffing, huffing, and bagging [2]. Sniffing involves direct inhalation from a container. Huffing is when a cloth is soaked in a substance and held over the mouth and nose. Bagging is when a paper or plastic bag is held over the face to maximize the concentration of the fumes. Hydrocarbons are lipophilic, which is important in both the central nervous system and the lungs. In the central nervous system, hydrocarbons are readily absorbed and act as depressants. They can cause free radical injury to the hippocampus, resulting in memory problems in chronic users, defined as using 2–3 times a week for 6 months [2]. In the lungs, hydrocarbons disrupt surfactant and thus decrease lung compliance. This disruption also causes inflammation, edema, and necrosis.
Our case is similar to two other cases of cardiomyopathy secondary to inhalant use [3,4]. In both of those cases, a spray called Dust-Off was used by the patients. A case of myocarditis has also been attributed to Dust-Off [5]. Unfortunately, our patient used a variety of hair sprays so it is impossible to know if a specific spray caused her symptoms. However, we assume that her symptoms were caused by hydrocarbon poisoning, as hydrocarbons are the active ingredients in most inhalants. Hydrocarbons increase the sensitivity of the cardiac myocardium to catecholamines, increasing the risk of arrhythmia [2]. Long-term use of hydrocarbons can cause myocardial degenerative changes such as intramyocardial hemorrhages, contraction band necrosis, ruptured myofibrils, and interstitial fibrosis. Our patient had a severe dilated cardiomyopathy that was likely secondary to a catecholamine surge. Based on the proposed mechanism of increased catecholamine sensitivity, one would expect to see a stress-induced cardiomyopathy with apical ballooning on echocardiography in the setting of inhalant use. However, in our case, as well as the two cited above, dilated cardiomyopathy developed. Additionally, our patient did not present with typical substernal chest pain, making Takotsubo cardiomyopathy less likely. Unfortunately, the patient has not been followed up, and we cannot assess if there was any improvement in her ejection fraction [3,4].
CONCLUSION
Inhalant abuse is prevalent mostly in teenagers but can continue into adulthood. Hydrocarbon solvents cause the ‘high’ but have detrimental effects on all organ systems. Of particular importance to this case is the effect that hydrocarbons have on the heart. Arrhythmia and heart failure should be considered in patients who present with chest pain or shortness of breath in the setting of inhalant abuse. Healthcare providers should be aware of this complication in patients with chronic inhalant abuse.