ABSTRACT
Introduction: Cocaine is a highly addictive substance that stimulates the sympathetic nervous system and cardiovascular system. A multitude of adverse cardiovascular events are associated with cocaine use including arrhythmia, congestive heart failure, coronary artery spasm and myocarditis.
Case Report: We present a rare case of Takotsubo cardiomyopathy after recent use of cocaine in a female without any other identifiable risk factor.
Discussion: Takotsubo cardiomyopathy (TCM) is a reversible cause of cardiomyopathy characterized by transient decrease in ejection fraction. Cocaine is a sympathomimetic that causes catecholamine surge and a variety of cardiovascular abnormalities. The association of cocaine use with Takotsubo cardiomyopathy is a rare occurrence, however the prognosis is generally good if diagnosis is made promptly.
Conclusion: Physician vigilance is required to diagnose this rare cause of cardiomyopathy and reduce morbidity and mortality.
LEARNING POINTS
- This case highlights the need to investigate the use of cocaine in patients with cardiovascular disease because it may influence the disease diagnosis and management strategies.
- Left heart catheterization is imperative for diagnosis, and cessation of cocaine is the primary goal of post discharge therapy.
- This case shows that TCM should be suspected in a patient with a history of cocaine use.
KEYWORDS
Cocaine, Takotsubo cardiomyopathy
INTRODUCTION
Takotsubo cardiomyopathy (TCM) is a rare condition that occurs as transient apical or mid-apical left ventricular dysfunction. This condition is often precipitated by emotional or physical stress [1]. The most plausible hypothesis is catecholamine cardiotoxicity that can cause subsequent stunning of the myocardium [2]. Although the trigger is mostly endogenous, some drugs have also been implicated in TCM. Cocaine is largely associated with myocardial ischemia and arrhythmia. We present a unique case of Takotsubo cardiomyopathy in a female without any other identifiable risk factor but with recent use of cocaine.
CASE DESCRIPTION
A 67-year-old female with a medical history of chronic obstructive pulmonary disease, hypertension and substance abuse presented to the emergency department with a complaint of chest pain for the past 3 days. Chest pain was left-sided, non-radiating, non-reproducible, localized to her left breast, 10/10 in severity. Pain worsened with exertion and was relieved with rest. It was associated with shortness of breath and sweating. The patient also complained of leg swelling for the past few days. She denied any history of cardiac workup in the past. She did not report significant family history of cardiac disease. The patient admitted to using cocaine via inhalation route in increased amount within the past few days. The patient denied any cough, palpitations, epigastric pain, headache, dizziness, abdominal pain, nausea or vomiting. On admission the patient was afebrile with blood pressure of 111/71 mmHg, heart rate of 77/min, respiratory rate 11/min and saturating 97% on room air. On cardiac examination, the rate and rhythm were regular with no murmur, rub or gallop. Bilateral lower extremity edema was present. The rest of the physical examination was unremarkable. Initial laboratory data showed elevated high sensitivity troponins with maximum value of 203 ng/L. The remainder of the laboratory parameters were unremarkable. Urine drug screen was positive for cocaine, opioids, benzodiazepines and methadone.
An electrocardiogram (EKG) showed sinus rhythm with normal axis, normal R wave progression and no significant ST-T wave changes. The patient was started on aspirin, high intensity statin, ticagrelor and heparin drip in the setting of elevated troponin. A transthoracic echocardiogram (TTE) showed left ventricular ejection fraction of 30-35% with severe hypokinesis of the entire mid- and apical walls (Fig. 1). Considering the echocardiogram findings and the patient’s persistent chest pain, left heart catheterization was performed. This showed nonobstructive coronary arteries with no coronary vasospasm (Fig. 2). With the absence of any obstructive coronary artery disease on cardiac catheterization, the TTE findings were consistent with Takotsubo/stress cardiomyopathy. Over the course of her hospital stay, the patient’s chest pain improved, and her condition stabilized. She was discharged on lisinopril, carvedilol, atorvastatin and aspirin. She was counseled to cease cocaine use. She was instructed to follow up with cardiology as out-patient. Cardiology follow-up at 60 days showed improvement in her clinical state and also echocardiogram findings.

Figure 1 (click to enlarge)
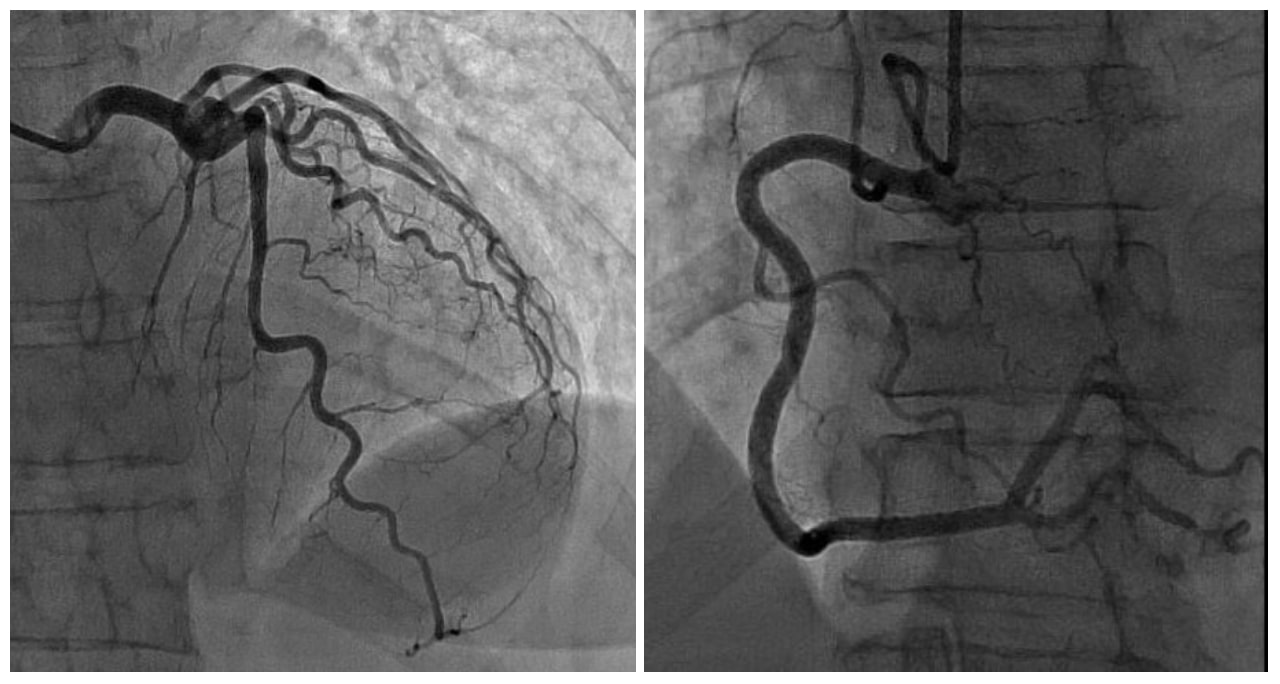
Figure 2 (click to enlarge)
Figure 1. Normal coronary angiogram
Figure 2. Severe hypokinesis of the apical walls on echocardiogram
DISCUSSION
Takotsubo cardiomyopathy (TCM) is a reversible cause of cardiomyopathy characterized by transient decrease in ejection fraction without the presence of coronary artery obstruction [3]. TCM which is also referred to as stress cardiomyopathy or left ventricular apical ballooning syndrome was first reported in Japan in 1991 by Sato et.al [4]. The pathophysiology behind TCM includes the sympathetic excitation of the central nervous system that triggers the release of catecholamines and results in apical systolic dysfunction and hyperdynamic basal contraction [5]. Several hypotheses have been proposed to describe the mechanism of TCM after a catecholamine surge, including myocardial injury caused either directly via cyclic AMP mediated calcium overload or indirectly by endothelial dysfunction and myocyte damage induced by catecholamine [6].
Cocaine is a highly addictive crystalline alkaloid that is the most frequent cause of drug-related deaths in the United States [7]. Cocaine mediates its effect by inhibition of norepinephrine, epinephrine, dopamine, and serotonin reuptake in the presynaptic neurons [7]. This causes overstimulation of alpha- and beta-adrenergic receptors. The resulting catecholamine surge is associated with a variety of cardiovascular abnormalities including myocardial infarction (MI), arrhythmia, cardiomyopathy and congestive heart failure [8]. Long-term cocaine use is associated with left ventricular hypertrophy and prolonged deceleration time [9]. The correlation between cocaine use and TCM can depend on factors such as the time of presentation in the hospital, illegal use and short half-life of cocaine, disparity in health care and other cardiac comorbidities pointing towards diagnoses with similar presentation. In our case the patient presented with chest pain a few days after consuming cocaine. Although a definite causal relationship cannot be ascertained, the close temporal association between the use of cocaine and the rapid onset of symptoms suggests that cocaine might be the trigger for the development of TCM. The echocardiogram having showed severe hypokinesis of the mid- and apical wall, and the left heart catheterization having showed no evidence of coronary artery disease, a diagnosis of TCM was made.
The treatment of TCM should be directed towards improvement of cardiac function and reduction of the risk of heart failure. Beta-blockers and angiotensin-converting enzyme inhibitors are generally used [5]. Counseling on drug addiction and detoxification are required since cessation of cocaine use have been shown to improve cardiac function. Our patient was discharged on aspirin, beta-blockers and angiotensin-converting enzyme inhibitors with counseling for cocaine cessation however she did not show up for her counseling appointment.
TCM is reversible and the prognosis is generally good if diagnosis is made promptly. Therefore, the possibility of TCM should be considered in patients with cocaine use who present with symptoms of acute chest syndrome with signs of ischemia on electrocardiography. Physician awareness about this rare association can reduce the mortality in TCM with early investigation and intervention like coronary angiography.