ABSTRACT
Thrombosis of the palmar digital veins is relatively rare, typically reported in women aged 35-65 years and most commonly occurring on the fourth digit. Clinical presentation varies and the lesion can present on the fingers or the palms of the hands. Diagnosis may be suspected clinically and confirmed on histology and radiologically. The condition can be managed conservatively or surgically. A 58-year-old woman presented with a 3-month history of a tender, skin-coloured nodule on her right palm. This was surgically excised, and the histopathological diagnosis was a thrombosed varix. As no underlying medical issues were raised on further testing, it was thought that her thrombosed varix was likely secondary to repeated trivial mechanical trauma, given that she was a housewife. A literature review yielded 36 cases of thrombosed varix, including our case. Most cases (85.3%) occurred in females, and the mean age of patients was 51.67 years, with two-thirds of patients between 35 and 65 years of age. The fourth digit and the proximal interphalangeal joint were the most commonly affected sites, respectively. Although rare, doctors should consider the possibility of a thrombosed varix when presented with tender and raised nodules on the palms or fingers.
LEARNING POINTS
- Thrombosis of the palmar digital veins is rare but can occur secondary to mechanical trauma and hypercoagulable states.
- Physicians should consider the possibility of a thrombosed varix when presented with a tender, raised and firm nodule on the hand or fingers, especially since some cases may be associated with hypercoagulable states which can have more serious sequelae.
KEYWORDS
Thrombosed varix, palmar digital vein, thrombosis, ultrasound Doppler, hypercoagulable state
CASE DESCRIPTION
A 58-year-old Caucasian woman presented to the Dermatology clinic with a 3-month history of a solitary, firm, tender and skin-coloured nodule in her dominant right palm, proximal to the third metacarpophalangeal joint (MCPJ). She denied recent trauma to the hands except for minor trivial injuries from household chores. Her medical history included osteoporosis, epilepsy, stage 2 chronic kidney disease and depression. She was a housewife, never smoked and denied recent illness or surgery.
An excision biopsy was performed, and histology revealed hyperkeratotic and acanthotic epidermis overlying an ill-defined nodule consisting of a large thin-walled vascular proliferation within which was a partly organizing thrombus, in keeping with a thrombosed varix (Figs. 1 and 2).
Laboratory blood tests including routine haematological and biochemical laboratory tests were unremarkable. A coagulation screen, including protein C activity, protein S activity, protein S free antigen, lupus inhibitor profile anticardiolipin, thrombin III activity, International Normalized Ratio (INR) and activated partial thromboplastin time (APTT) was normal. Given the histological diagnosis, the patient was referred to vascular surgery and underlying arteriovenous malformations were excluded with an ultrasound Doppler examination of the hands.
The patient was seen again 1 month after the procedure. On examination she had a well-healed scar (Fig. 3) and no further complaints.

Figure 1 (click to enlarge)
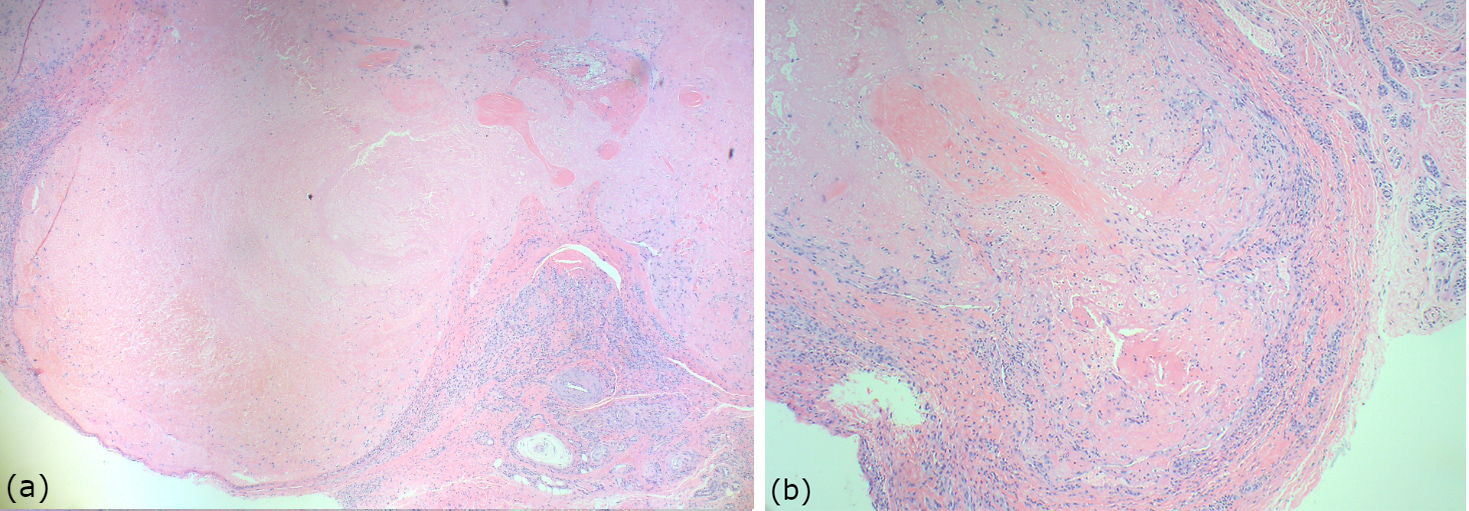
Figure 2 (click to enlarge)

Figure 3 (click to enlarge)
Figure 1. Low-power view of the acral skin and the superficial part of a thrombosed dilated vascular channel (haematoxylin and eosin (H&E) stain ×40)
Figure 2. MRI of the thoracic spine showing long segments of increased cord signal with T2–T7 involvement
Figure 2. Low- (a) and high- (b) power views showing the thrombosed varix in the deep dermis (haematoxylin and eosin (H&E) stain ×40 and ×200, respectively)
Figure 3. The patient's surgical scar 1 month after excision of her thrombosed varix
DISCUSSION
Thrombosis of the palmar digital veins is relatively rare, with only 35 cases reported in the literature since it was first described by Jadassohn in 1936, making our case the 36th. An extensive literature research was carried out to identify all reported cases of thrombosed varices of the palmar digital veins and to determine patient characteristics including demographic details, site/s affected, underlying causes and management. PubMed and Google Scholar were used to search for these cases, using the terms ‘thrombosed varix’ and ‘palmar digital vein’. Search results are summarized in Tables 1 and 2.
Table 1 (click to enlarge)
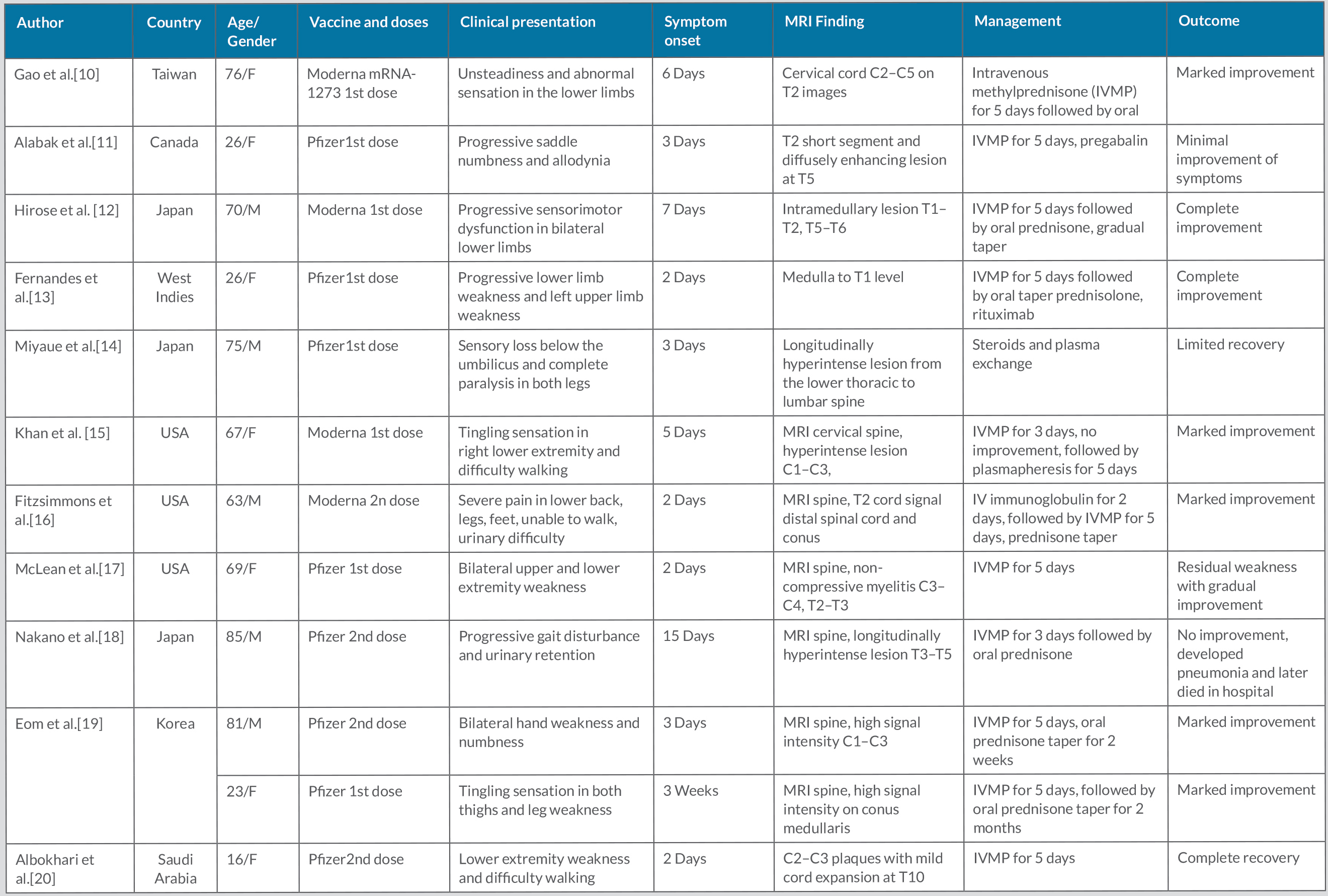
Table 2 (click to enlarge)
Table 1. Overview of cases of thrombosed varix of the hand reported in the literature
D, digit; DIPJ, distal interphalangeal joint; F, female; M, male; N, no; NS, not stated; OCP, oral contraceptive pill; PIPJ, proximal interphalangeal joint; Y, yes.
Table 2. Results of a literature review of 36 cases of thrombosis of the palmar digital veins
DIPJ, distal interphalangeal joint; PIPJ, proximal interphalangeal joint
Of the 34 patients whose gender was reported, 85.3% (n=29) were female and 14.7% (n=5) male. Gender was not given in the remaining two patients. Age was specified in 33 patients, the majority (66.7%, n=22) of whom were 35–65 years of age. The mean age of the reported cases was 51.67 years (range 27–81 years).
Thrombosis usually manifests as solitary or multiple papules or nodules[1]. Our review found the fourth digit was affected 17 times and In addition to our case, the palm was the site of a thrombosed varix only twice; one case was secondary to an underlying hypercoagulable state[2] and the other to mechanical trauma [3].
The lesions are commonly bluish but may also be erythematous [4] or skin-coloured [5], especially if the lesion is deep enough and the overlying skin is thicker or hyperkeratinised.
Hand dominance was only reported in 13 cases, including ours. All these patients were right hand dominant, with six having the thrombosed varix on their right hand and the remaining seven on the left hand. Therefore, hand dominance does not seem to influence the side affected. Moreover, in three other cases, the lesions occurred on both hands, with these patients all having underlying hypercoagulable states.
Digital vein thrombosis lesions may present with tenderness. This may be quite bothersome for patients as it can interfere with daily activities. Our patient had complained of pain, which was the main reason for her presentation. In our review, we found that tenderness was reported in 19 patients (76%), but that the lesions were painless in six other patients (24%).
Thrombosis commonly occurs in the superficial axial veins of the palmar aspect of the digits [1]. The aetiology is still uncertain, although possible contributing factors may be related to the anatomy of the palmar digital veins. The palmar veins are small in diameter, are enclosed in fine connective tissue and fat, and have more valves than the dorsal digital veins. These features increase their susceptibility to collapse with advancing age and, coupled with repeated mechanical trauma with compression to the hands, increase the risk of thrombus formation [1]. In our case, the only plausible trigger was repeated trivial mechanical trauma from household chores, given that the patient was a housewife. Trauma was also noted to be the most common trigger in our case series: of the 23 cases in which an underlying cause was reported, documented trauma was the potential cause for the thrombosis in 12 cases (52.2%). This was secondary to household chores, as well as gardening, sewing and some occupations.
Inherited or acquired hypercoagulable states may also give rise to thrombosis of the palmar veins, with 8 out of 23 (34.8%) reported cases being secondary to hypercoagulable states. Documented causes included recurrent venous thromboembolism since adolescence of uncertain aetiology [2], isolated high levels of IgM antiphospholipid antibodies [6] and factor V Leiden mutation [7], recent surgery to the upper limb [1] and malignancy (prostate cancer) [8]. Drugs known to increase the risk of venous thromboembolic events, namely hormonal treatment including the combined oral contraceptive pill [9] and the intrauterine device containing levonorgestrel, have also been reported[6]. More recent possible triggers for palmar vein thrombosis include COVID-19 infection [7] and the COVID-19 vaccine. The latter was reported 8 days after vaccination with a first dose of the Oxford-AstraZeneca COVID-19 vaccine [10].
Thrombosis was reported to be spontaneous in three (13%) of the reported cases. However, it is possible that a thrombosed varix seems spontaneous in origin but is due to mechanical trauma. This may be the case with Lanzetta and Morrison [11] and Spies [12] where the thrombosis was deemed to be spontaneous although the authors noted that the patients did manual activities such as golfing, household chores or manual labour.
The underlying cause for thrombosed varix formation was not specified in 13 cases.
Diagnosis of a thrombosed varix may be based on clinical findings, however it is not always clear since other conditions such as haemangiomas and non-thrombosed varicosities may have a similar presentation. A Penrose tourniquet placed at the base of the digit may help to distinguish between a thrombus, haemangioma and a non-thrombosed varix. A thrombus would not engorge, while a haemangioma and a non-thrombosed varix would do so [1]. Ultrasound or magnetic resonance imaging [13] may also be considered to exclude other causes of palmar nodules such as epidermal cysts, lipomas, ganglion cysts, fibromas of the tendon sheath, schwannomas and possibly sarcomas [14]. Surgical excision with biopsy is another option. In our case, the patient underwent surgical excision in the first instance due to the pain and the clinical diagnostic uncertainty.
Thrombosed varices may be managed medically and surgically. In our review, 18 patients (60%) were treated surgically and 11 (36.7%) medically. One patient (3.33%) was treated both medically and surgically [2]. In the remaining six cases, the type of management was not specified. Conservative treatment included massaging the nodule and hot compresses [15]. In the case of thrombosis secondary to hypercoagulable states, treatment also included compression bandaging [2], aspirin [2] and rivaroxaban [10]. Surgical excision is almost always curative and considered when the lesion is causing discomfort to the patient or if the clinical diagnosis is uncertain [15]. Its dual purpose for diagnosis and treatment could explain why surgery was the most common treatment option.
CONCLUSION
To our knowledge this is the third reported case of a thrombosed varix on the palm of the hand. Physicians should consider the possibility of a thrombosed varix when presented with a tender, raised and firm nodule on the hand or fingers. Although in themselves not life-threatening, some cases may be associated with hypercoagulable states which can have more serious sequelae.