ABSTRACT
Intrathoracic kidney is a very rare finding, representing less than 5% of all renal ectopias. Because of the location of the liver, thoracic kidney on the right side is much less common than thoracic kidney on the left side. Although an increasing number of case reports are being published in the literature, few describe the impact of the ectopia on kidney function. We report the case of a woman with intrathoracic right kidney and chronic kidney disease that was initially misdiagnosed as pneumonia because of its presentation on chest x-ray. We highlight the need to including this condition in the differential diagnosis[2] as the literature rarely links it to changes in kidney function.
LEARNING POINTS
- Intrathoracic kidney is an extremely rare condition that should be considered in the differential diagnosis of intrathoracic masses.
- There is a lack of literature on this type of kidney ectopia and its consequences in asymptomatic individuals.
KEYWORDS
Intrathoracic kidney, chronic kidney disease
CASE DESCRIPTION
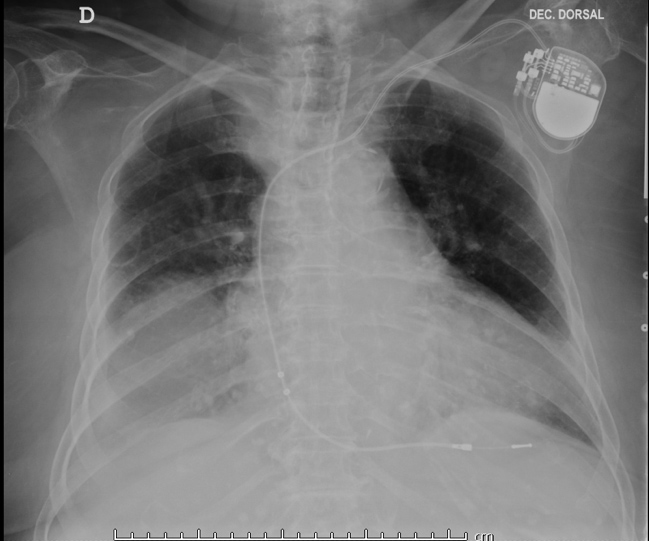
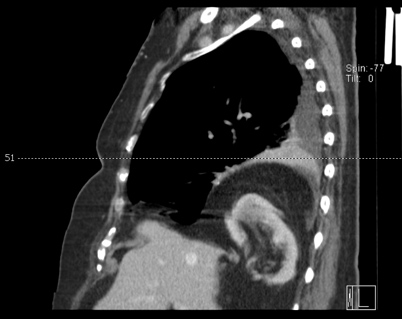
An 89-year-old widow was brought by her daughter to the Emergency Department due to an altered state of consciousness and weakness, but no history of falls or trauma. Her medical history showed arterial hypertension treated with perindopril and amlodipine, chronic kidney disease, diabetes mellitus treated with pioglitazone and glimepiride, pacemaker implantation, and peripheral arterial occlusive disease. The results of her physical examination revealed mild dehydration and decreased vesicular murmur in the base of the right lung. Blood tests revealed acute-on-chronic kidney disease (serum creatinine 2.9 mg/dl), hyperkalaemia (5 mmol/l), blood urea nitrogen 100 mg/dl, and C-reactive protein 70 mg/dl (normal range <5 mg/dl). Chest x-rays showed a rounded radio-opacity in the lower part of the right hemithorax (Fig. 1). Because of these findings, the patient was admitted to the Internal Medicine department with the diagnosis of pneumonia and started on empirical antibiotics and fluid support. There was a significant improvement in renal function, which returned to its basal range (serum creatinine 1.9 mg/dl), and potassium levels were normalized. Due to the unavailability of previous chest images, a chest CT scan (Figs. 2 and 3) was performed that revealed a diaphragmatic right posterior hernia with herniation of the epiploic fat and the right kidney without signs of renovascular stenosis or hydronephrosis. Because of the patient’s age and the absence of complaints, hernia repair was not recommended. The patient was discharged with a follow-up appointment.
(click to enlarge)
Figure 1. Chest x-ray showing homogenous well-defined right lower opacity

(click to enlarge)
Figure 2. CT chest scan (coronal section) showing a diaphragmatic right posterior hernia measuring approximately 12×8 cm, with intrathoracic herniation of epiploic fat and the right kidney
(click to enlarge)
Figure 3. CT chest scan (sagittal section) showing intrathoracic herniation of epiploic fat and the right kidney
DISCUSSION
While the majority of thorax radio-opacities are due to common diseases, such as pneumonia, in cases with an unclear presentation a thorough study should be performed and rare causes considered. We do not recommend detailed investigation in every case, but the lack of fever and respiratory complaints in this patient suggested further examination. The patient had undergone pacemaker implantation 10 years previously, but we did not have access to the relevant chest images. We hypothesize the patient´s kidney ectopia could have been caused by a congenital diaphragmatic hernia that may have enlarged with time allowing the kidney to herniate further into the thoracic cavity. The vast majority of congenital diaphragmatic hernias are detected and corrected in childhood, which is one of the reasons why the long-term prognosis of this condition is poorly defined.[1,4]
Our case was interpreted as an incidental finding and since the patient’s comorbidities such as hypertension and diabetes mellitus could have caused her chronic kidney disease, we are not able to determine if the kidney ectopia was a contributing factor. Although renal ectopia may predispose to renal disease or complicate surgical procedures and pregnancy, it is also compatible with a long asymptomatic life, as in our patient.[3]
Due to the rarity of this condition and because most of the literature on kidney ectopia is from a surgical point of view, guidelines are lacking on how to follow-up asymptomatic patients. Nevertheless, the recommended approach is a wait-and-see strategy while monitoring symptoms and kidney function.[1]