ABSTRACT
Introduction: Epipericardial fat necrosis (EFN) is a relatively rare benign disease that causes acute chest pain.
Case Description: A woman in her 20s presented with acute left shoulder and epigastric pain. One day before presentation, she had visited a cardiologist and an acute coronary syndrome had been ruled out. The pain worsened with deep inspiration. Chest computed tomography (CT) showed a soft-tissue attenuation lesion containing a fatty centre located in the epipericardial fat at the left cardiophrenic angle. Hence, EFN was diagnosed and the pain was resolved with loxoprofen. The lesion had disappeared on a follow-up chest CT scan.
Discussion: EFN is a rare benign disease that causes acute chest pain. Approximately 70–90% of EFN cases are misdiagnosed by clinicians as other diseases.
Conclusion: In patients with acute chest pain, the correct diagnosis of EFN avoids unnecessary invasive investigations and reassures patients.
LEARNING POINTS
- Patients with epipericardial fat necrosis typically present with acute pleural chest pain without any associated symptoms.
- Characteristic CT findings of the encapsulated fatty pericardial lesion with a surrounding inflammatory reaction are key for the diagnosis of epipericardial fat necrosis.
- The correct diagnosis of epipericardial fat necrosis in patients with acute chest pain reassures them and avoids unnecessary invasive investigation.
KEYWORDS
Epipericardial fat necrosis, chest pain, mediastinal tumour
CASE DESCRIPTION
A woman in her mid-20s presented with a 1-week history of left shoulder and epigastric pain. The patient was asymptomatic until 7 days before presentation when she developed pain in the left shoulder and epigastric pain. One day before presentation, she had visited a cardiologist. Although acute coronary syndrome and acute pericarditis were considered differential diagnoses, the results of cardiac troponins, electrocardiography and chest radiography suggested a low possibility of these diagnoses.
Since the pain persisted and the patient was not diagnosed, she visited our outpatient clinic in the general internal medicine department for further investigation. The pain worsened with deep inspiration, but the patient denied any other symptoms, including upper back pain, palpitations, dyspnoea and nausea. Her medical history included Wolff-Parkinson-White syndrome, meniscus injury, and oral contraceptive usage. However, there was no family history of cardiovascular disease. Currently, the patient is a smoker with 2.5 pack-year history and is an occasional drinker. Additionally, she is allergic to shiitake mushrooms.
METHODS AND PROCEDURES
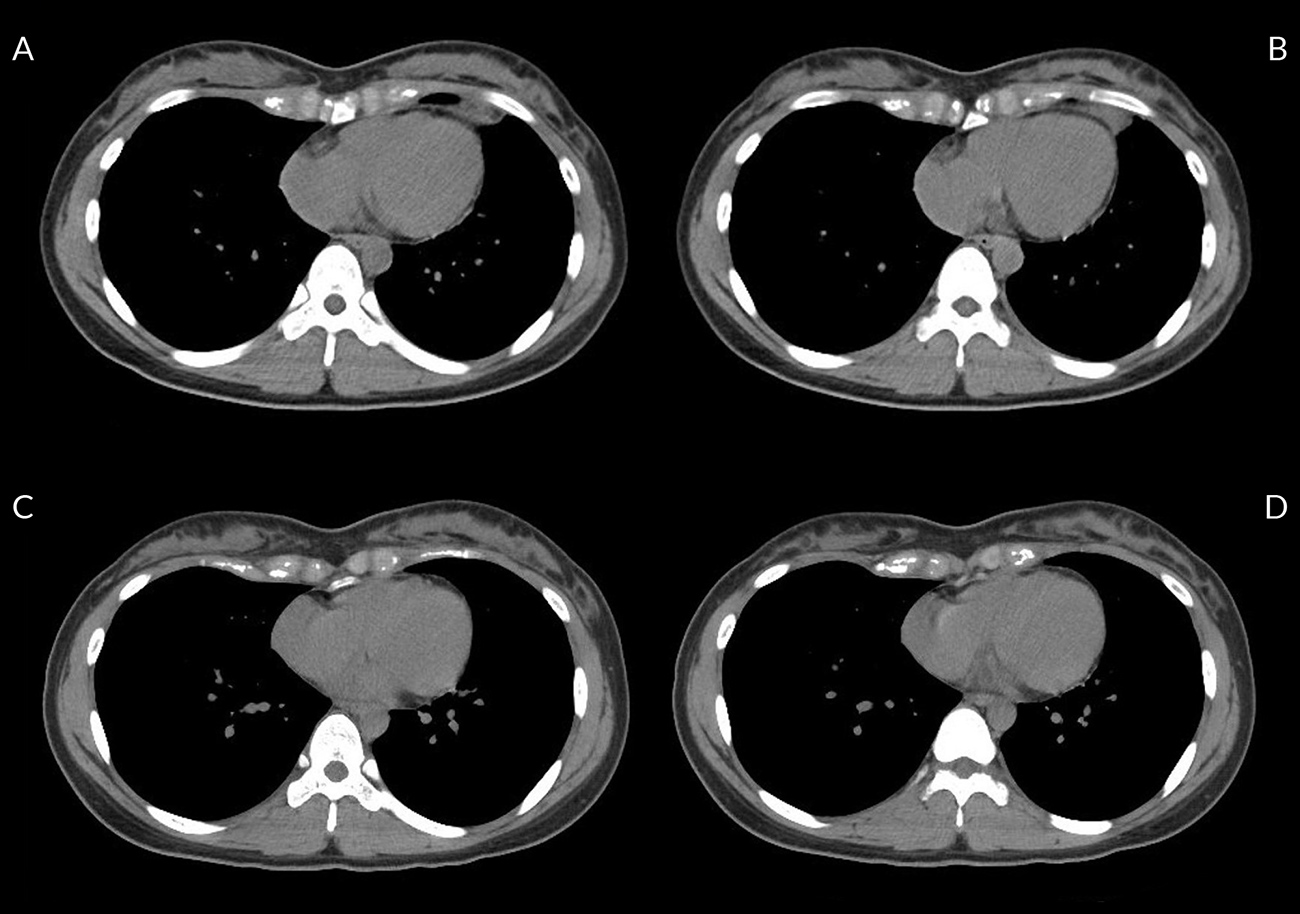
On physical examination, the patient’s vital signs were normal. No erythema or tenderness was observed in the left shoulder or epigastric area. Chest auscultation revealed no friction rubs, murmurs or respiratory crackles. Although slightly increased white blood cell counts (9,400 mm3/l) and slightly elevated C-reactive protein levels (0.79 mg/dl) were noted, cardiac troponin and D-dimer levels, chest radiography and electrocardiography were normal. A non-contrast chest computed tomography (CT) scan revealed a soft-tissue attenuation lesion containing a fatty centre located in the epipericardial fat at the left cardiophrenic angle (Fig. 1A,B). We diagnosed the patient with epipericardial fat necrosis (EFN) based on the clinical symptoms and imaging findings. Subsequently, her pain resolved within 1 week with loxoprofen, and the pericardial lesion had disappeared on a follow-up chest CT scan 3 months after presentation (Fig. 1C,D).
(click to enlarge)
Figure 1. (A, B) Chest CT scan at the presentation shows a soft-tissue attenuation lesion that contains a fatty centre located in the epipericardial fat at the left cardiophrenic angle. (C, D) Follow-up chest CT scan 3 months after presentation reveals disappearance of the soft-tissue lesion.
DISCUSSION
EFN is a rare benign disease that causes acute chest pain and was first described by Jackson et al. in 1957[1]. EFN is a self-limiting cause of acute chest pain[2], which can be detected in 2.2–2.8% of chest CT scans performed for acute chest pain[3,4]. Patients with EFN typically present with acute pleural chest pain without associated symptoms[2,3]. EFN has no specific findings on blood tests or electrocardiograms, and chest x-rays may be normal. Hence, the characteristic CT findings of an encapsulated fatty pericardial lesion with surrounding inflammatory reactions are key for diagnosis[2]. Approximately 70–90% of EFN cases may be misdiagnosed by clinicians as other conditions[3,4]. The correct diagnosis of EFN is significant as it reassures patients and avoids over-investigation since there are broad differential diagnoses for acute epigastric pain (e.g., acute coronary syndrome, acute pericarditis, pulmonary thromboembolism, pneumonia, cholecystitis, cholangitis, peptic ulcer disease). EFN usually resolves within 1–2 weeks without any specific treatment[2], but a follow-up CT scan within 2–3 months may be recommended to exclude the possibility of a tumour[4].