ABSTRACT
Hydatid disease, also known as cystic echinococcosis, is a parasitic infection caused by the larval stage of Echinococcus granulosus. It usually invades organs such as the liver and the lungs but can affect any organ. Isolated cardiac involvement is a rare manifestation. We present a case of isolated left ventricle hydatid cyst with negative serological tests, which was treated with surgical removal and confirmed by histopathological examination.
LEARNING POINTS
- Isolated cardiac hydatid disease is rare and accounts for only 0.5–2% of cases among infected patients.
- Cardiac hydatidosis may present with a wide variety of clinical manifestations ranging from no symptoms to sudden death; palpitations may be the only complaint.
- Surgical excision is the treatment of choice for cardiac hydatid disease to avoid high-risk complications.
KEYWORDS
Hydatid cyst, cardiac echinococcosis, echocardiography
INTRODUCTION
Isolated cardiac echinococcosis is a rare manifestation of cystic echinococcosis that may be asymptomatic or manifest in various ways. It can be detected by different imaging modalities, serological tests, or histopathological examination of the removed specimen. We present the case of a 47-year-old woman who presented with intermittent palpitations and was found to have a cystic mass in the left ventricle (LV) with no other organs affected. Serological tests were negative, but on histopathological examination after surgical removal, the mass was found to be an isolated cardiac hydatid cyst.
CASE DESCRIPTION
A 42-year-old woman, with no significant history of medical or surgical problems, presented with several weeks’ history of intermittent palpitations with no other complaints. Her physical examination was normal, her family medical history was negative, and her personal medical history was unremarkable for medications or allergies.
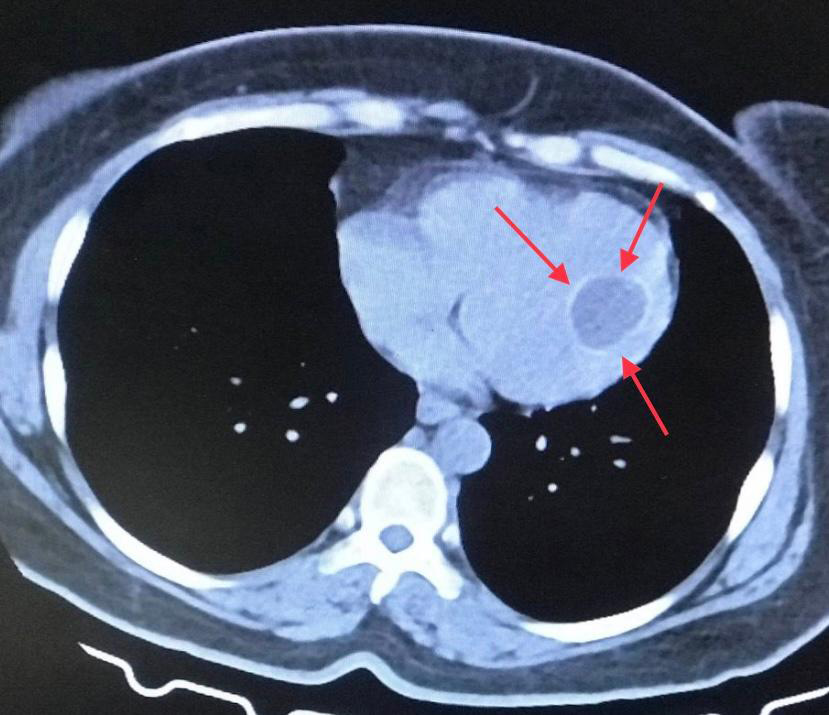
The chest x-ray did not show any lung lesions. Her electrocardiogram showed non-specific changes. She was referred for echocardiography, which showed an oval-shaped mass inside the LV attached to the anterolateral wall (Fig. 1). The mass had a cystic appearance with a thick wall measuring 4.5×3.5 cm. The size of the LV and systolic function were normal, and there was no evidence of inflow obstruction through the mitral valve. The echocardiographic picture raised the suspicion of a hydatid cyst. Her contrast-enhanced computed tomography (CT) scan showed a well-defined cystic mass located inside the LV (Fig. 2). CT did not identify any other lung or mediastinal lesions. Abdominal-pelvic ultrasonography was also negative for any cystic lesions. Laboratory data showed normal liver and renal function tests and complete blood count. The serological test to detect antibodies with enzyme-linked immunosorbent assay (ELISA) was also negative.
Figure 1. Transthoracic echocardiography (apical four-chamber view) of the cystic mass with a thick wall attached to the anterolateral wall of the LV (red arrow). LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle

(click to enlarge)
Figure 2. Computed tomography image showing a well-defined cystic mass located inside the left ventricle (red arrows)
(click to enlarge)
Figure 3. The cystic mass after surgical removal
The patient was started on albendazole therapy and was scheduled for cardiac surgery for the excision of the cystic mass. To reduce the risk of spillage of cyst contents during the procedure, surgical excision was performed under cardiopulmonary bypass. A cystic mass measuring 4.5×3×2.5 cm was completely removed (Fig. 3). Pathological examination confirmed the diagnosis of a hydatid cyst. Postoperative echocardiography showed an LV without any masses and only mild hypokinesia of the mid-anterolateral wall. The patient was discharged home on the fourth day postoperatively. She was later seen in a follow-up visit in an outpatient clinic and was in good health with no more palpitations.
DISCUSSION
Echinococcosis is a parasitic disease caused by infection with tiny tapeworms of the genus Echinococcus and is classified as either cystic or alveolar echinococcosis. Hydatid disease is endemic in cattle-rearing areas of the world, notably Mediterranean countries, the Middle East, South America, Australia and New Zealand, and remains a public health, economic and social problem[1]. The most common primary site of hydatid cysts is the liver (60%–70%), followed by the lungs (10%–15%), muscles (5%), bones (3%), kidneys (2%), spleen (1%) and brain (1%)[2]. Infections in humans are usually asymptomatic, with slowly enlarging cysts in the liver, lungs and other organs that often grow unnoticed and go neglected for years. Cardiac involvement in infected patients accounts for only 0.5–2% of cases, and is considered a rare manifestation of the disease[3].
The most common pathway for cardiac invasion by the parasitic larvae is via the coronary circulation: the hexacanth embryos of the parasite released from the ova escape from the vascular beds of the liver and lungs and travel to the myocardium. This pathway may explain why 55%–60% of hydatid cysts are located in the LV since it is rich in coronary supply[4]. Other cardiac locations of hydrated cysts are less common with 10%–15% of cysts found in the right ventricle, 7% in the pericardium and pulmonary artery, 6%–8% in the left atrium, 3%–4% in the right atrium, and only 4% in interventricular septum[4]. Cysts in the ventricular walls can grow (at approximately 1 cm per year) either towards the epicardium or the endocardium, which results in growth into the pericardial cavity or intracavitary space.
Cardiac echinococcosis infection clinically may have a wide range of manifestations, ranging from no symptoms to sudden death. The different clinical manifestations of cardiac hydatid cysts are mostly related to the size, number, location and integrity of the cysts, and the presence of complications[5]. A ruptured cardiac hydatid cyst can lead to pericardial effusion with subsequent acute cardiac tamponade[5]. Systemic embolism, when the cyst is located in the left ventricular outflow tract, or pulmonary embolism, when it is located in the right ventricular outflow tract[6], arrhythmias and valvular dysfunction can also be manifestations of cardiac echinococcosis. Anaphylactic shock is a dramatic consequence of a ruptured cardiac hydatid cyst in the bloodstream. Acute stroke due to cardiac hydatidosis is extremely rare, and only a few cases have been reported in the literature[7]. The most common arrhythmia associated with cardiac hydatid disease is ventricular tachycardia and high-grade atrioventricular block[8]. Chest pain is the most frequent symptom, while palpitations, cough and dyspnoea are less common[9]. Palpitations as the only symptom for cardiac hydatid disease is a rare presentation.
In endemic or agricultural areas, cardiac echinococcosis should be kept in mind as a potential differential diagnosis when non-specific clinical symptoms in addition to suspected intracavitary masses are encountered. The cystic-like mass may have a uni‑ or multicystic appearance macroscopically and is usually filled with fluid containing small daughter cysts and hydatid sand[10]. In endemic areas, the diagnosis of cardiac hydatid cysts requires a high suspicion and is usually based on the results of imaging techniques and specific serological tests to detect antibodies against Echinococcus granulosus[11]. ELISA is the most specific serological test to detect these antibodies[12], where a positive result helps confirm the diagnosis, although a negative test cannot rule out the diagnosis. Transthoracic echocardiography is the preferred initial diagnostic tool as it can determine the presence of cystic masses, their number, location and size, and the possible involvement of other adjacent anatomical structures[2]. Additional useful diagnostic tools include CT and magnetic resonance imaging (MRI)[13], which help localize and define the morphological features of hydatid cysts, including cardiac localization. CT best shows wall calcification, while MRI depicts the exact anatomic location and nature of the internal and external structures.
Surgery remains the treatment of choice to manage cardiac hydatid disease. Medications have been used preoperatively and postoperatively since 1977, but surgical removal of the hydatid cyst under cardiopulmonary bypass is recommended[14,15]. The risk of spillage of cardiac cyst contents was minimized when the cardiopulmonary bypass technique was utilized during resection[16]. In some reports, an off-pump technique was used to remove superficially located cysts[17]. In inoperable cases, administration of albendazole can reduce the size of cysts and halt their development[18].
Our patient demonstrated isolated cardiac involvement of hydatid disease manifested with palpitations only, with negative serology for antibodies. The diagnosis was confirmed on histopathological examination of the resected cyst. Surgical treatment was the treatment of choice in our case to avoid high-risk complications.
CONCLUSION
Cardiac hydatidosis is rare and may present with a wide variety of clinical manifestations. Surgical excision is the treatment of choice to avoid high-risk complications.
- Salih OK, Celik SK, Topcuoglu MS, Kisacikoglu B, Tokcan A. Surgical treatment of hydatid cysts of the heart: a report of 3 cases and a review of the literature. Can J Surg 1998;41:321–327.
- Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev 2004;17:107–135.
- Gençpınar T, Guzeloglu M, Aykut K, Albayrak G, Hazan E. A rare localization of hydatid cyst: right ventricular free wall cyst fistulized to the ventricular cavity. J Cardiovasc Surg 2013;1:13–15.
- Niarchos C, Kounis GN, Frangides CR, Koutsojannis CM, Batsolaki M, Gouvelou-Deligianni GV, et al. Large hydatic cyst of the left ventricle associated with syncopal attacks. Int J Cardiol 2007;118:e24–6.
- Fazlinezhad A, Moohebati M, Azari A, Bigdeloo L. Acute pericardial tamponade due to ruptured multiloculated myocardial hydatid cyst. Eur J Echocardiogr 2009;10:459–461.
- Orhana G, Bastopcua M, Aydemirb B, Ersoz MS. Intracardiac and pulmonary artery hydatidosis causing thromboembolic pulmonary hypertension. Eur J Cardiothorac Surg 2018;53:689–690.
- Cakir O, Eren N, Kilinc N. Cardiac hydatic cyst causing cerebral emboli in a child. Pediatr Cardiol 2002;23:555–556.
- Dong Z, Yusup M, Lu Y, Tang B. Hydatid cyst of the heart as a rare cause of arrhythmia: a case report and review of published reports. HeartRhythm Case Rep 2022;8:458–462.
- Pakis I, Akyildiz EU, Karayel F, Turan AA, Senel B, Ozbay M, et al. Sudden death due to an unrecognized cardiac hydatid cyst: three medicolegal autopsy cases. J Forensic Sci 2006;51:400–402.
- Gurzu S, Beleaua MA, Egyed‑Zsigmond E, Jung I. Unusual location of hydatid cysts: report of two cases in the heart and hip joint of Romanian patients. Korean J Parasitol 2017;55:429–431.
- Kahlfuß S, Flieger RR, Roepke TK, Yilmaz K. Diagnosis and treatment of cardiac echinococcosis. Heart 2016;102:1348–1353.
- Sağlıcan Y, Yalçın Ö, Kaygusuz E. Cystic echinococcosis: one entity, two unusual locations. Turkiye Parazitol Derg 2016;40:51–53.
- Narin N, Mese T, Unal N, Pinarli S, Cangar S. Pericardial hydatid cyst with a fatal course. Acta Paediatr Jpn 1996;38:61–62.
- Onursal E, Elmaci TT, Tireli E, Dindar A, Atilgan D, Ozcan M. Surgical treatment of cardiac echinococcosis: report of eight cases. Surg Today 2001;31:325–330.
- Gormus N, Yeniterzi M, Telli HH, Solak H. The clinical and surgical features of right-sided intracardiac masses due to echinococcosis. Heart Vessels 2004;19:121–124.
- Miralles A, Bracamonte L, Pavie A, Bors V, Rabago G, Gandjbakhch I, et al. Cardiac echinococcosis. Surgical treatment and results. J Thorac Cardiovasc Surg 1994;107:184–190.
- Rossouw GJ, Knott-Craig CJ, Erasmus PE. Cardiac echinococcosis: cyst removal in a beating heart. Ann Thorac Surg 1992;53:328–329.
- Dumitru IM. Medical treatment of cystic echinococcosis. In: Derbel F, Braiki M, editors. Overview on echinococcosis. London: IntechOpen, 2019.