ABSTRACT
Light-chain (AL) amyloidosis is the most common type of amyloidosis; cardiac involvement is rare but has a poor prognosis. Biventricular hypertrophic cardiomyopathy is an exceptional finding in amyloidosis and its association with obstructive right ventricular gradient is even rarer. We report the case of a male patient with biventricular hypertrophy suggesting amyloidosis, with an obstructive gradient in the right ventricle.
LEARNING POINTS
- Consider amyloidosis in a patient presenting with signs of congestive heart failure and low or microvoltage on ECG.
- It is important to examine right ventricle myocardium thickness, as hypertrophy not only occurs in the left ventricle, and look for a right ventricle outflow tract gradient.
- Analysis of speckle tracking of the myocardium will show deterioration of the basal and medium segments with normal apical segment motion.
KEYWORDS
Biventricular hypertrophic cardiomyopathy, right ventricle outflow tract, amyloidosis, low voltage
INTRODUCTION
Biventricular hypertrophic cardiomyopathy (HCM) is an uncommon condition that is caused in most cases by systemic infiltrative disease. Its association with an obstructive right ventricular gradient is even rarer. We report the case of a male patient with biventricular hypertrophy suggesting amyloidosis with an obstructive gradient in the right ventricle.
CASE REPORT
A 62-year-old man was admitted to our clinic with exertional dyspnoea and swelling of the lower limb. Physical examination revealed a systolic ejection murmur and signs of congestive heart failure. The electrocardiogram (ECG) showed typical microvoltage (Fig. 1). Transthoracic echocardiography (TTE) revealed severe biventricular hypertrophy (Fig. 2) and a maximum right ventricle outflow tract gradient of 36 mmHg at rest (Fig. 3). Colour Doppler imaging did not show left ventricular outflow obstruction, aortic stenosis, aortic coarctation or signs of cardiac shunt. Strain analysis showed typical normal longitudinal strain values at the apical segments of the left ventricle, and reduced strain at all basal segments, suggesting amyloidosis (Fig. 4). Biopsy of salivary glands confirmed the diagnosis of AL amyloidosis. The patient died suddenly from cardiac arrest.
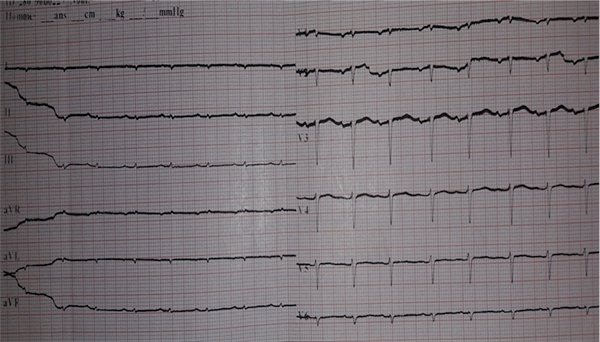
Figure 1 (click to enlarge)
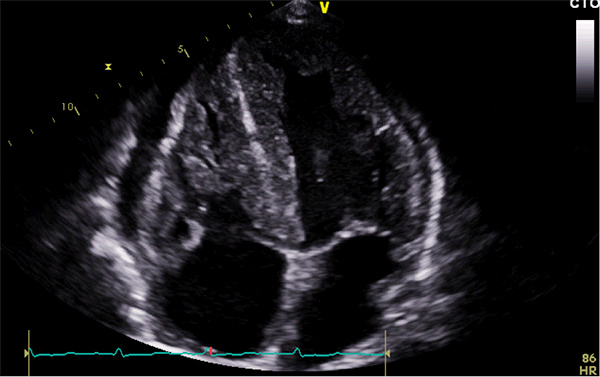
Figure 2 (click to enlarge)
Figure 1. 12-Lead ECG showing typical microvoltage
Figure 2. TTE revealing severe biventricular hypertrophy and a granular and sparkling appearance of the myocardium
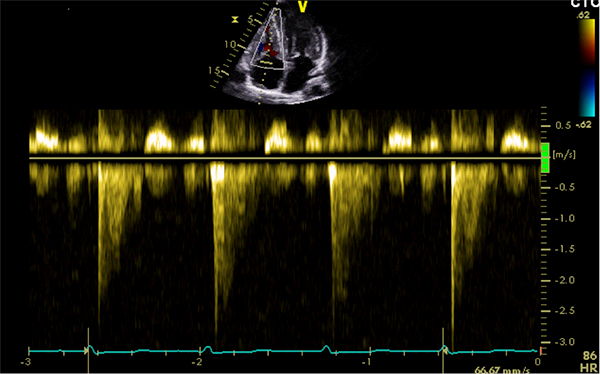
Figure 3 (click to enlarge)
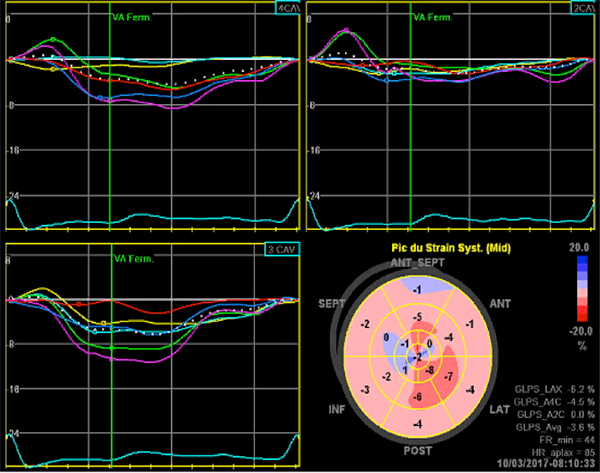
Figure 4 (click to enlarge)
Figure 3. TTE showing a maximum gradient of 36 mmHg at rest
Figure 4. Bull's eye mapping analysis showing a normal longitudinal strain value at the apex of the left ventricle (bright red), and significantly reduced strain at all basal segments of the entire left ventricle (pale pink to light red)
DISCUSSION
AL amyloidosis is the most common type of amyloidosis; cardiac involvement is rare but remains the main prognostic factor[1]. When heart failure occurs, death can result within 4–6 months[2]. The aim of this report is to remind clinicians to always consider amyloidosis in a patient with signs of congestive heart failure and a low or microvoltage on ECG. ECG remains the best test to assess HCM and the presence of outflow tract obstruction. In the majority of systemic infiltrative diseases, hypertrophy most commonly affects the left ventricle, causing left ventricle outflow tract obstruction (LVOT). LVOT seems to be due to dynamic and mitral valve systolic anterior motion[3]. In this report, we describe the very rare condition of biventricular hypertrophy with right ventricle obstruction. This condition is extremely uncommon and results from excessive muscular hypertrophy[4]. Analysis of speckle tracking of the myocardium showed typical normal longitudinal strain values at the apex of the left ventricle, and reduced strain at all basal segments, suggesting amyloidosis. Prognosis in amyloidosis is strongly related to the presence of ECG abnormalities: septal wall progression, left ventricle dysfunction and impaired gradient peak velocity[5].