ABSTRACT
We describe a 58-year-old woman presenting with headache and an elevated erythrocyte sedimentation rate (ESR), who was diagnosed with and successfully treated for giant-cell arteritis (GCA). Seven months after the end of treatment, ovarian GCA was incidentally found after ovariectomy for a simple cyst. GCA of extracranial vessels like the ovarian arteries is rare. Nevertheless, we stress that extracranial GCA should be considered in patients older than 50 years with an elevated ESR, even if a temporal artery biopsy is negative or specific symptoms are absent. Moreover, we discuss the importance of imaging techniques when GCA of the extracranial large vessels is suspected.
LEARNING POINTS
- Although rare, ovarian arteries can be involved in giant-cell arteritis (GCA).
- Extracranial GCA should be considered in the differential diagnosis of patients aged 50 years or older with an elevated ESR, even if temporal artery biopsy is negative or specific symptomatology of GCA is absent.
- If GCA is suspected but the origin is unclear, an MRA or PET-CT scan should be performed to screen for GCA of extracranial arteries.
KEYWORDS
Giant-cell arteritis, ovarian arteries, rare manifestation, vasculitis in female genital tract
CASE DESCRIPTION
In April 2010, a 58-year-old woman, with a history of nicotine abuse and a simple ovarian cyst, presented with severe headache (without tenderness of the temporal artery), malaise and an elevated erythrocyte sedimentation rate (ESR) of 107 mm in the first hour (normal <20 mm/hour). CRP and liver enzyme levels were normal. Oral prednisolone therapy (30 mg daily) was started by her general physician. However, as her complaints persisted while being treated for several weeks, she was referred to the hospital. The clinical and laboratory parameters, in particular the patient's age (>50 years old), the new onset of the headache and the increased ESR, fulfilled at least three classification criteria for giant-cell arteritis (GCA)[1]. The issue of a late temporal artery biopsy (TAB) to prove GCA, taking into account the pretreatment, was discussed, but a TAB was refused by the patient. A positron emission tomography (PET)-CT scan was also not performed, as this was not yet part of the standard work-up for GCA at that time. Since the suspicion of GCA was nevertheless high, the oral prednisolone therapy was continued, now using an increased dosage of 60 mg daily. During 6 weeks of high-dose prednisolone treatment, the ESR normalized (19 mm/hour) and the headache decreased. However, upon tapering of the prednisolone, the severe headache and elevated ESR (68 mm/hour) immediately returned. Therefore, prednisolone was further tapered, and a subsequent prolonged, steroid-sparing treatment with methotrexate (10 mg daily for 10 months) was initiated. As a result, the ESR again normalized and the headache, after still being intermittently present during the first months, finally resolved. Seven months after the end of treatment, a laparoscopic bilateral ovariectomy was performed in order to remove a slowly growing simple ovarian cyst. Histological examination showed, in addition to a benign ovarian cyst, an infiltrate of lymphocytes, macrophages and giant cells in the walls of the hilar arteries of both ovaries, indicative of ovarian artery GCA (Fig. 1A,B). Since the patient did not have any complaints postoperatively, further treatment was not required.
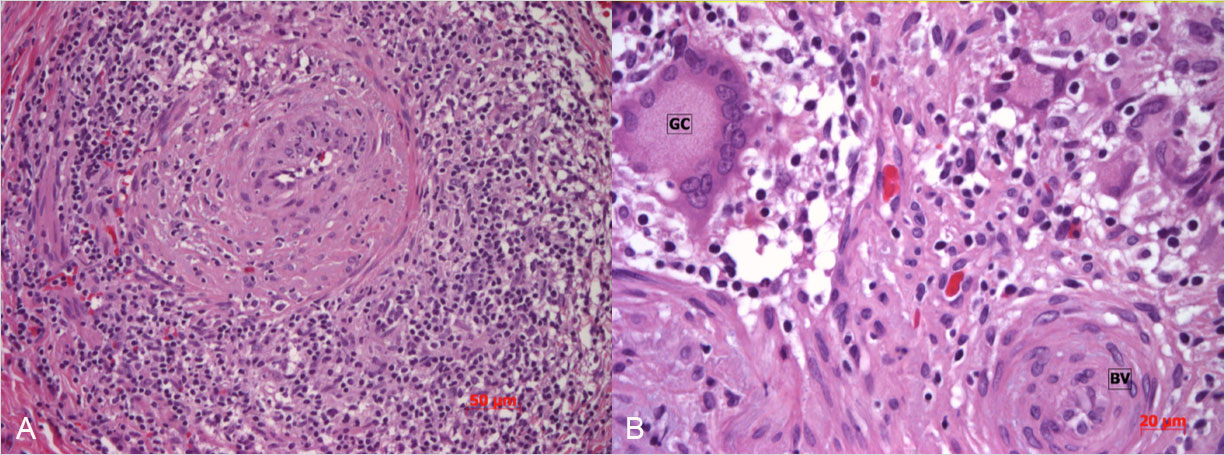
Figure 1 (click to enlarge)
Figure 1. Histopathological examination of the ovarian tissue showed a giant-cell arteritis of the ovarian arteries, characterized by (A) a dense infiltrate and (B) multiple giant cells (GC) in the wall of the blood vessel (BV)
DISCUSSION
GCA is a systemic vasculitis of medium- to large-sized arteries, typically involving the temporal artery (temporal arteritis)[2,3]. GCA is the most common form of systemic vasculitis in adults, with an annual incidence of 20 per 100,000 individuals among Northern Europeans above 50 years of age[4]. GCA is caused by dendritic cells in the vessel wall, recruiting T-cells and macrophages to locally form a granulomatous infiltrate, characterized by giant cells (fused macrophages)[5]. GCA most commonly involves the superficial temporal artery, but it can also affect the carotid arteries, the vertebral arteries, the subclavian, axillary and proximal brachial arteries, the ascending aorta and the coronary arteries[3]. Less frequently involved are the descending aorta and mesenteric, renal, iliac and femoral arteries[4]. Rarely, GCA of the arteries of the lungs, cervix, breast or ovaries is found (see supplementary references 1–4). Symptoms may include headache, tenderness of the scalp, jaw claudication, tinnitus, diplopia, and, if occlusion of the ophthalmic artery occurs, the feared complication of sudden and irreversible blindness[2, 3]. Systemic manifestations like fever, fatigue and malaise may also be present[6]. While clinical and laboratory parameters can raise suspicion, a TAB is needed for a definitive diagnosis of GCA[3]. GCA is treated with high-dose prednisolone, or alternatively with methotrexate or azathioprine[4].
The above-described case of GCA is remarkable, since GCA of the ovarian arteries is rare and has only sporadically been reported before (see supplementary references 5–13). Also in the few previous reports, GCA of the ovarian arteries was detected incidentally, by histopathological examination after an ovariectomy for a lesion unrelated to GCA. In general, most of the incidental GCA discoveries concerned GCA in the female gynaecological tract or in the breasts (see supplementary references 2–13). Presumably, this is partly due to the high number of mastectomies, hysterectomies and ovariectomies performed.
Since, in our case, the patient presented with new-onset headache, the suspicion of GCA was quickly raised and treatment was immediately started. However, in most of the previously reported cases of GCA in the female genital tract, patients were either asymptomatic or experiencing vague systemic manifestations like malaise, fever, anaemia and weight loss. In these patients, the diagnosis was not considered until GCA was coincidentally found in surgically removed tissue, and consequently the appropriate treatment was only started a long time after the initial complaints. Moreover, there may be patients with gynaecological GCA who have never been diagnosed (since they did not undergo surgery) and therefore have not been treated at all. Of note, treatment does not seem to be required in patients with gynaecological GCA who are asymptomatic[7].
As mentioned previously, a TAB is necessary to diagnose GCA. However, in up to 42% of the GCA patients with extracranial large-vessel manifestation, TAB is negative[8]. Therefore, if GCA is suspected, but the clinical criteria are not fulfilled and/or the TAB is negative, PET-CT is needed to investigate whether one or more of the above-described arteries are affected by GCA. Importantly, PET-CT is only able to detect inflammatory vessel wall disease of the larger arteries[9]. MRA can be used to look for stenosis in the smaller vessels (although it cannot discriminate between arteritis and atherosclerosis)[3].
In our patient, an active infiltrate was found within the ovarian artery walls despite prior extensive treatment. Previous studies showed that corticosteroid treatment usually improves the clinical symptoms and laboratory values, but often fails to eliminate the vascular inflammation[10]. Still, it could be argued from clinical experience that current corticosteroid treatment regimens are sufficient to prevent most of the vascular complications and systemic manifestations of GCA[10].
In conclusion, besides its well-known manifestation in the temporal artery, GCA can be present at many other sites of the body, such as the female genital tract. Therefore, extracranial GCA should be considered in the differential diagnosis of patients aged 50 years or older with an elevated ESR, even if TAB is negative and specific symptomatology of GCA is absent. The imaging tools of PET-CT and MRA, which are widely available nowadays, have become important aids in the diagnosis of rare presentations of GCA.