ABSTRACT
Immunoglobulin G4-related disease (IgG4-RD) is a systemic immune-mediated fibroinflammatory condition characterized by tumefactive lesions that can affect multiple organs. Serum IgG4 levels may be elevated. Early recognition is sometimes difficult but is important to avoid irreversible organ damage. We describe the case of a 28-year-old male patient who presented with a 2-year history of recurrent low-grade fever, night sweats and non-specific manifestations. We eventually diagnosed IgG4-related aortitis by PET-CT scan. The patient was successfully treated with prednisolone and mycophenolate mofetil with complete clinical and radiological resolution.
LEARNING POINTS
- IgG4-related disease is a systemic immune-mediated disease that can affect many organs and systems.
- Aortitis can be one of the differential diagnoses in patients with fever of unknown origin, back pain and other unspecific symptoms.
- Delayed diagnosis and treatment may cause major complications or irreversible damage, so timely diagnosis and appropriate treatment is very important.
KEYWORDS
IgG4-related disease, aortitis, glucocorticoids, fever of unknown origin
CASE PRESENTATION
We describe the case of a 28-year-old man referred to our internal medicine department by primary care. He presented with an 18-month history of recurrent nocturnal low-grade fever of about 37.5–38° accompanied by chills and night sweats. The patient had experienced persistent left back pain and left upper quadrant abdominal pain for 3 months, without urinary or other gastrointestinal symptoms. He also reported easy fatigability but denied anorexia or significant weight change. His past medical history was unremarkable except for minor thalassaemia. He was not a smoker, and denied alcohol abuse or illicit drug use. On evaluation in the outpatient setting, he was alert, oriented, cooperative and afebrile. His blood pressure was 115/72 mmHg, pulse was 105 beats per minute, and respiratory rate was 18 breaths per minute. The rest of the physical examination was unremarkable. A complete blood count revealed microcytic hypochromic anaemia (haemoglobin of 9.6 g/dl, mean corpuscular volume of 73.6 fl, mean corpuscular haemoglobin of 24.0 pg), and white blood cells and platelets within the normal range. However, he had a high C-reactive protein level of 9.96 mg/dl and a high erythrocyte sedimentation rate of 100 mm/h, an elevated ferritin level of 530.3 ng/ml, complement 3 and complement 4 levels of 1.90 g/l (slightly increased) and 0.31g/l (normal), respectively, and high serum IgA, IgG and IgG4 levels of 11.77 g/l, 30.45 g/l and 1.412 g/l, respectively. Serum urea, creatinine, liver enzymes, transferrin, vitamin B12, rheumatoid factor, tumour markers and thyroid profile were normal, and 24-hour urine protein was negative. Tests for immune markers such as antinuclear antibodies (ANA), anti-neutrophil cytoplasmic antibodies (ANCA), LE cells, lupus anticoagulants and anticardiolipin antibody were negative. Other tests, such as HIV type 1 and type 2 antibodies, interferon gamma assay, and blood cultures for bacteria and mycobacteria were negative. Computed tomography (CT) of the chest, abdominal and pelvic area was unremarkable except for mild splenomegaly. The haematology department was consulted for an expert opinion; a trephine bone marrow biopsy was performed and revealed normocellular bone. A PET-CT scan was then requested and showed increased 18FDG uptake at the aortic arch, ascending aorta and thoracic descending aorta, left carotid artery and right subclavian/axillary artery (Fig. 1). Treatment with 30 mg prednisolone and 1,000 mg mycophenolate mofetil per day was initiated with immediate clinical improvement. The patient is currently completely symptom free. A follow-up PET-CT scan showed significantly decreased FDG uptake at the previous aortic lesions (Fig. 2. The serum IgG4 level also declined to the normal range. A cardiology consultation was requested and excluded coronary artery involvement.
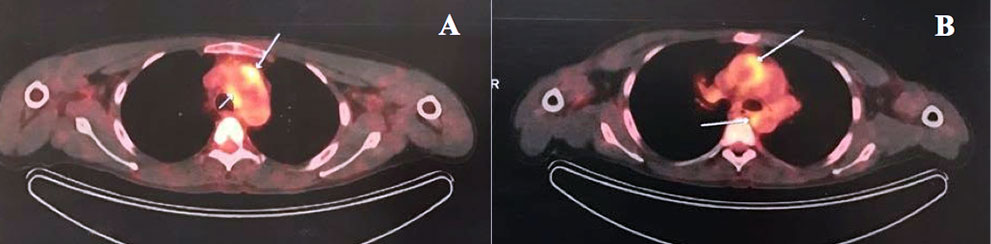
Figure 1 (click to enlarge)
Figure 1. PET-CT images showing increased 18FDG uptake at the aorta. (A) Aortic arch lesion; (B) ascending aortic and descending aortic lesions

Figure 2 (click to enlarge)
Figure 2. PET-CT image 3 months after initiation of treatment. The image shows resolution of inflammation and no abnormal 18FDG uptake at the aortic arch, ascending aorta or descending aorta
DISCUSSION
Immunoglobulin G4-related disease (IgG4-RD) is a systemic immune-mediated fibroinflammatory condition and systemic disorder that links many individual organ conditions previously considered to be unrelated[1,2]. It is more commonly found in men between the sixth and seventh decades of life with sex-dependent clinical manifestations reported[1,2]. However, clinical manifestations can be highly non-specific and dependent on the involved organs[3]. There are no standard laboratory parameters for diagnosis and the serum IgG4 level is considered to have a low positive predictive value. However, some have reported that this may be due to the ‘prozone effect’ and suggested high diagnostic accuracy if used correctly. Imaging studies are mainly employed for differential diagnosis, with 18F-FDG PET-CT being a useful assessment tool[4]. Histopathology is the gold standard and should be utilized whenever possible[2]. Glucocorticoids are the first-line agent for remission induction in all patients with active, untreated IgG4-RD unless contraindications are present[1].
Cardiovascular system involvement includes arteritis, periarteritis, pericarditis and pseudotumours around the coronary arteries[5]. Large vessel involvement in IgG4-RD is not common, with incidence ranging from 9% to 22.5%. However, IgG4-related cardiovascular diseases can be easily overlooked and not diagnosed in a timely manner due to the non-specific clinical manifestations. Some reported cases have resulted in irreversible damage or significant complications such as myocardial ischaemia, dissection, rupture or tamponade[5]. The diagnosis is even more challenging when the disease only affects the cardiovascular system with no tumefactive lesions in other organs. Secondly, the diagnostic criteria for IgG4-related disease include IgG4-positive plasma cell infiltration in specific organs. However, it is usually difficult to obtain a pathological specimen for patients with suspected IgG4-related cardiovascular disease unless surgical or endovascular intervention is performed for the purpose of treatment. In these circumstances, 18F-FDG PET-CT is a helpful tool for assessing organ involvement and disease distribution[4]. It can guide the choice of more accessible disease-involved biopsy sites, such as the salivary glands, rather than the cardiovascular system. However, although there is no evidence of salivary gland involvement, some articles have suggested that gland biopsy can be electively performed simultaneously or afterwards since it is the most commonly affected organ. However, the advantages and disadvantages of the procedure should be discussed thoroughly with the patient.
Steroid therapy remains the first-line treatment for IgG4-related disease[1]. Some biomarkers for IgG4-RD have been described, including plasmablasts, which are considered to correlate well with disease activity. However, these markers are not widely used and their efficacy as predictors of disease flare-up requires further study.