
Keywords
ST-segment elevation myocardial infarction, recurrent myocardial infarction, early recurrence of myocardial infarction, STEMI
Abstract
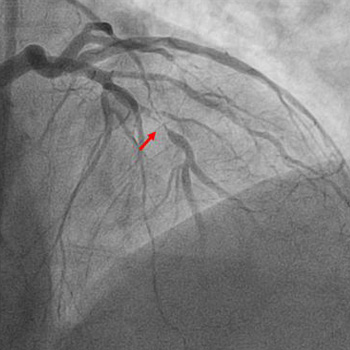
An acute ST-elevation myocardial infarction (STEMI) followed by reinfarction within a short period of time is typically due to stent thrombosis. However, a STEMI caused by occlusion of one vessel followed by a repeat infarction due to occlusion of a different vessel which was seemingly innocent a few hours earlier is extremely rare. We present the case of a 61-year-old male with a past medical history of prediabetes, hyperlipidemia, tobacco use, and gastroesophageal reflux disease who presented to the emergency department with complaints of chest pain. His initial electrocardiogram (EKG) revealed ST elevation in leads II, III and aVF with reciprocal changes in leads I and aVL. He promptly underwent cardiac catheterization and had percutaneous coronary intervention with placement of two drug-eluting stents (DES) in the right coronary artery (RCA). At that time coronary angiography revealed 50% stenosis of the left anterior descending (LAD) artery and 60% stenosis of the second diagonal branch artery. Shortly after the procedure he was asymptomatic, and the post procedure EKG demonstrated resolution of the ST elevations. However, within 2 hours he developed chest pain and was found to have new ST elevations in the anterolateral leads. Repeat cardiac catheterization revealed patent RCA stents with subtotal occlusion of the LAD and another DES was placed. After the second procedure the patient remained hemodynamically stable, EKG changes resolved, and he was kept on eptifibatide infusion for 18 hours after which he was switched to dual antiplatelet therapy and ultimately discharged home.
References
Views: 49
PDF downloads: 29
HTML downloads: 21
Published:
2024-04-03
Issue:
2024: LATEST ONLINE
(view)






