EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 0
HTML: 0
PDF: 0
|
Ischaemic colitis is responsible for more than half of the presentations of gastrointestinal ischaemia and develops due to an interruption of intestinal blood flow. Risk factors include increasing age and conditions associated with decreased perfusion. Infrequently, ischaemic colitis may develop in young females prescribed oral contraceptives. Here, we present a case of ischaemic colitis secondary to oral contraceptives that resolved with medication discontinuation.

|
Views: 257
HTML: 30
PDF: 145
|
Introduction: Polymyalgia rheumatica (PMR) is a chronic inflammatory disorder that causes stiffness and pain in the proximal joints, including the shoulders, hips and neck. The exact cause of polymyalgia rheumatica is yet to be fully understood, but research suggests that both genetic and environmental factors may contribute to it. Studies have previously linked the onset and relapse of polymyalgia rheumatica symptoms to the influenza and COVID-19 vaccines. The Food and Drug Administration approved the respiratory syncytial virus (RSV) vaccine, which is a recombinant protein vaccine for adults over 60, in May 2023. No previous reports of polymyalgia rheumatica onset or relapse have been linked to the RSV vaccine. The human proteome shares some peptides with the RSV F antigen, suggesting a high risk of cross-reactivity when using that antigen in vaccination formulations.
Case description: A 72-year-old man experienced a new onset of bilateral shoulder pain and stiffness three days after receiving the Abrysvo® RSV vaccine. The symptoms lasted more than an hour (up until noon) and interfered with his activities of daily living. Inflammatory markers such as C-reactive protein were elevated. The patient’s symptoms and inflammatory marker levels significantly improved with prednisone therapy.
Conclusion: In patients with typical PMR symptoms, it is important for clinicians to carefully review immunisation history to rule out any potentially related adverse effects.

|
Views: 187
HTML: 32
PDF: 129
|
We describe a rare case of polyserositis with chylous ascites following nivolumab therapy, highlighting the challenges in recognizing and managing immune-related adverse events (irAEs) associated with immune checkpoint inhibitors (ICPIs).

|
Views: 328
HTML: 51
PDF: 237
|
Neutropenia by non-chemotherapy drugs is an extremely rare idiosyncratic life-threatening drug reaction. Ceftriaxone and meropenem are widely used broad-spectrum antibiotics and are generally safe and well tolerated. The authors present a case of neutropenia induced by ceftriaxone and meropenem in an adult patient. The resolution of neutropenia occurred within 48 hours of ceftriaxone and meropenem being discontinued. Although antibiotic-induced neutropenia is uncommon, clinicians should be mindful of this adverse drug effect because of its potential development of severe neutropenia, septicaemia, septic shock, deep-seated infections and even death. Therefore, neutropenic sepsis treatment should be initiated without delay, particularly if the patient becomes septic and febrile. Granulocyte-colony stimulation factor (G-CSF) may be administered to facilitate the recovery process with daily monitoring of neutrophil count. Mortalities from antibiotic-induced neutropenia remain rare, with a range of 2.5–5%.

|
Views: 166
HTML: 24
PDF: 105
|
Khat is a plant that is commonly used for its stimulating effects and is chewed for its psychoactive properties. It creates feelings of euphoria that are similar to when taking amphetamines. There is an association between khat and liver injury, but the mechanism is not well known. We present three cases of khat-induced liver injury. All cases have elevated IgG and either positive antinuclear antibodies (ANA) or anti-smooth muscle antibody (ASMA); each case has a different course and requires different management. One case improved only by stopping khat, one required a short course of steroids and the last case required treatment such as that for autoimmune hepatitis (AIH).

|
Views: 437
HTML: 24
PDF: 201
|
Background: Vaccine-induced immune thrombotic thrombocytopenia (VITT) is a rare life-threatening thrombotic reaction to COVID-19 vaccines.
Case description: Two young male first cousins, with a family history of idiopathic thrombocytopenic purpura, developed VITT after the Ad26.COV2.S vaccine. Both had a favourable clinical and analytical outcome. We investigated the genetic factors that could be associated with a genetic predisposition to VITT.
Conclusions: There are no published cases where the VITT patients were relatives. The genetic study did not reveal any likely pathogenic variants, although the prevalent polymorphism c.497A>G (p.(His166Arg)) in the FCGR2A gene was found in a homozygous state. More studies are required to better understand VITT’s pathophysiology and any underlying genetic predispositions.

|
Views: 476
HTML: 26
PDF: 313
|
Euglycemic diabetic ketoacidosis (euDKA) is a rare but severe metabolic complication of diabetes mellitus characterised by elevated anion gap metabolic acidosis despite normal or mildly elevated blood glucose levels. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have emerged as effective antidiabetic medications, yet their use is associated with an increased risk of euDKA, especially when coupled with insulin dose reduction.
We present the case of a 50-year-old male with a 20-year history of diabetes mellitus, initially managed with insulin and metformin, who developed euDKA following the introduction of empagliflozin and sitagliptin alongside a reduction in insulin therapy. Despite normoglycaemia the patient exhibited symptoms of ketoacidosis, including chronic fatigue, polydipsia, and polyuria.
Diagnostic workup revealed metabolic acidosis, elevated inflammatory markers, acute kidney injury and ketonuria. Subsequent specialised laboratory tests confirmed type 1 diabetes mellitus (T1DM) with the presence of anti-glutamic acid decarboxylase (anti-GAD) antibodies and the absence of C-peptide secretion. Management involved fluid therapy, intravenous insulin and glucose administration.
This case underscores the diagnostic challenges of euDKA and emphasises the importance of differentiating between T1DM and T2DM, as management strategies vary significantly. Patient education on insulin therapy and injection techniques is crucial to prevent complications such as improper insulin delivery and dose reduction, which can precipitate euDKA.
In conclusion, clinicians should be vigilant for euDKA in patients on SGLT2 inhibitors, particularly when insulin dose reduction is involved. Comprehensive patient education and accurate differentiation between diabetes types are essential for timely diagnosis and optimal management, thereby reducing the risk of severe complications.
|
Views: 403
HTML: 236
PDF: 471
|
Background: Studies have shown major cardiovascular effects associated with ketamine use disorder including dose-dependent negative inotropic effects. Preoperative ketamine use has been linked to ketamine-induced stress cardiomyopathy.
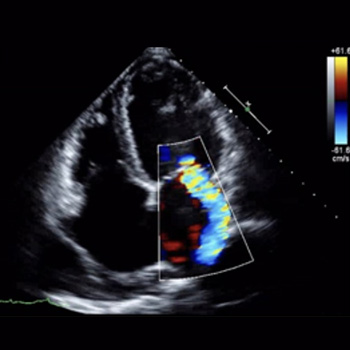
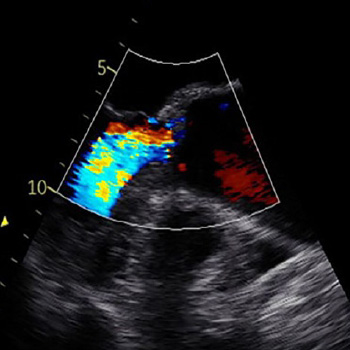
Case presentation: A 28-year-old female with a history of recurrent cystitis and ketamine use disorder (twice weekly for 14 years) presented with bilateral lower extremity oedema and shortness of breath for 3 months. She was tachycardic with a troponin level of 0.07 ng/ml and a B-type natriuretic peptide (BNP) level of 2511 pg/ml. Electrocardiogram showed normal sinus rhythm and transthoracic echocardiography (TTE) showed left ventricular ejection fraction (EF) of 15%, dilated left ventricle, and severe tricuspid and mitral regurgitation. Computed tomography (CT) scan of the chest and abdomen showed bilateral pleural effusions with congestive hepatopathy and ascites. The patient was started on intravenous furosemide, metoprolol, and sacubitril/valsartan. Rheumatological workup including complement levels, and antinuclear anti-double-stranded DNA was negative. A repeat TTE 2 weeks later revealed an EF of 25% and moderate tricuspid regurgitation. Four months later, the EF was 54% with normal left ventricular cavity size.
Conclusion: Although ketamine use disorder is increasing, data on long-term side effects is minimal. Screening for ketamine use disorders should be considered in patients presenting with acute systolic heart failure. Long-term studies are needed to evaluate the benefits of adding ketamine screening to standard urine toxicology.
|
Views: 273
HTML: 15
PDF: 248
|
Case description: We describe a case of a patient treated with pembrolizumab (an immune checkpoint inhibitor) for metastatic scalp melanoma. He had a previous history of colorectal cancer, prostatic cancer and chronic polymyalgia rheumatica. The patient was known to have a stable ascending aortic aneurysm of 4.5 cm. However, he developed a rapid expansion of the ascending aortic aneurysm with the size crossing the threshold for surgery. The patient was referred to the cardiothoracic surgery service for intervention and he subsequently underwent surgery. The patient was electively admitted one week later for resection of aortic aneurysm, aortoplasty and external graft fixation. Pathologically, gross evidence of dissection was not identified; however, the histological analysis of the media showed laminar medial necrosis, multifocal in nature, with occasional clusters of histiocytic cells appreciated at their edge reminiscent of that seen in an inflammatory aortitis (granulomatous/giant cell type).
Discussion: Immune checkpoint inhibitor-induced aortitis is becoming increasingly evident, and its presentation can vary. It has been discovered incidentally on surveillance imaging with the use of nivolumab. In other cases, patients have been symptomatic to severely symptomatic. Atezolizumab with carboplatin and etoposide has been reported to cause abdominal aortitis which was responsive to corticosteroids and subsequent discontinuation of atezolizumab. Pembrolizumab has been linked to a case of transverse aortic arch aortitis. In our case, the inflammatory aortitis due to pembrolizumab was the cause of the rapid expansion of the ascending aortic aneurysm.
Conclusion: Patients with known aortic aneurysms should undergo careful surveillance when commencing immune-checkpoint inhibitor therapy.

|
Views: 186
HTML: 10
PDF: 164
|
Introduction: Sudden onset of reduced consciousness, psychomotor agitation and mydriasis are all indicative of an anticholinergic toxidrome. It is important to note that numerous drugs, as well as certain herbs and plants, possess anticholinergic properties.
Case description: An 84-year-old female patient had sudden nocturnal onset of uncoordinated hand movements and altered mental status. Shortly after, the patient’s 83-year-old husband developed symptoms of dysarthria, gait ataxia, vertigo, and delirium.
Conclusion: Anticholinergic syndrome consists of a combination of central and peripheral anticholinergic symptoms. Physostigmine given intravenously resulted in rapid reversal of symptoms. Thorn apple seeds had been accidentally ingested and were identified as the cause.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

