EJCRIM 2023 CiteScore
| 2.1 = | 1.751 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by




|
Views: 0
PDF: 0
HTML: 0
|
The incidence of post-infectious autoimmune diseases has been on the rise following the COVID-19 pandemic. Recently, an autistic patient was admitted to the hospital presenting with a mild upper respiratory system COVID-19 infection. Months after recovery and polymerase chain reaction negativity, the patient developed HEp-2 cell positivity and presented with relapsing polychondritis (RP), a rare autoimmune disease. The mechanism of this autoimmune invasion is ultimately caused by activating a myriad of immune reactions. Lymphocytopenia almost always accompanies various clinical forms of COVID-19; however, it may drive the lymphocytopenia-induced proliferation of autoreactive T cells via the activation of interleukin-6 (IL-6). Moreover, high levels of neutrophils during infection promote autoimmune disease by releasing cytokine and chemokine cascades that accompany inflammation, and neutrophil extracellular traps regulating immune responses through cell–cell interactions. Furthermore, autism spectrum disorder patients display an altered immune system that includes an augmented inflammatory cytokine milieu leading to an increased pro-inflammatory Th1/Th2 ratio. In addition, the pathophysiology of RP is majorly associated with a cell-mediated immune reaction; thus, the predisposing exaggerated immune system of such patients must also be considered as a predisposing factor to the development of post-infectious autoimmune diseases.

|
Views: 18
HTML: 1
PDF: 6
|
Late onset combined immunodeficiency (LOCID) is a rare variant of common variable immunodeficiency (CVID), typically affecting adult patients who present with opportunistic infections (OI) and/or low CD4+ T lymphocytes. Diagnostic delay is common due to the rareness of this entity, increasing morbidity and mortality. We report on a 66-year-old male who developed a severe gastrointestinal cytomegalovirus (CMV) infection, refractory to antiviral treatment and anti-cytomegalovirus specific human immunoglobulin administration, with a fatal outcome due to an undiagnosed LOCID.

|
Views: 56
HTML: 4
PDF: 16
|
Introduction: Blue rubber bleb nevus syndrome is a rare disorder of venous malformations, with around 200 cases reported. We present a case of Mycobacterium xenopi infection in a patient with blue rubber bleb nevus syndrome.
Case Description: A 40-year-old female with blue rubber bleb nevus syndrome, asthma, and bronchiectasis came to the pulmonology clinic with shortness of breath and a cough. She was recently admitted for a bronchiectasis exacerbation but continued to have a worsening productive cough and fevers. The most recent CT scan of the chest showed interval stable right upper lobe fibrocavitary disease, demonstrating gradual progression over two years. She had occasional positive cultures for Mycobacterium Avium Complex and M. xenopi one year previously, assumed to be a colonizer and not treated. Most recent hospital cultures were negative for bacteria and an acid-fast bacilli smear. She was sent to the emergency department for bronchiectasis exacerbation and returned to the clinic six weeks later with two sputum cultures growing M. xenopi. It was decided to treat M. xenopi as this was likely the cause of her cavitary lung lesion and frequent infections. Azithromycin, rifampin, and sulfamethoxazole/trimethoprim were initiated. Intravenous amikacin was added later on. She finally had a right partial lung resection done after one year at an outside hospital. She was on and off antibiotics for M. xenopi for approximately three years with negative repeat cultures for non-tuberculous mycobacteria.
Conclusion: Due to the high mortality of M. xenopi infections (which can be as high as 69%), treatment of at least twelve months is recommended. To our knowledge, this is the first reported case of M. xenopi in a patient with blue rubber bleb nevus syndrome.

|
A rare case of biloma after ascending cholangitis and endoscopic retrograde cholangiopancreatography
Views: 42
HTML: 7
PDF: 17
|
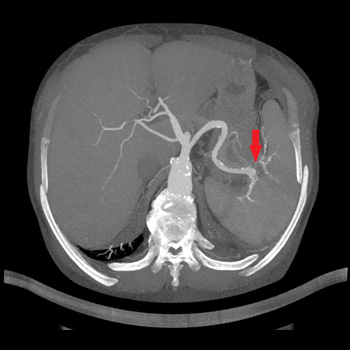
Introduction: Biloma is an uncommon form of liver abscess composed of bile usually associated with procedures of the biliary tree and gallbladder. Cholangitis can be acute or chronic, can result in partial or complete obstruction of the flow of bile. The infection of the bile is so common, that positive blood cultures are highly characteristic. In the case of a suppurative cholangitis with signs of sepsis treatment alone with antibiotics is usually not sufficient to achieve medical remission. Multiple hepatic abscesses are often present, and the mortality approaches 100% unless prompt endoscopic or surgical relief of the obstruction and drainage of infected bile are carried out. Endoscopic retrograde cholangiopancreatography ERCP with endoscopic sphincterotomy is the preferred initial procedure for both establishing a definitive diagnosis and providing effective therapy.
Case description: We present the case of a 69-year-old female patient with complex chronic comorbidities who presented with acute cholangitis initially managed with endoscopically inserted stent and later complicated by sepsis and biloma formation. The bile was drained, and it showed an infection with Candida spp. requiring antifungal therapy.
Conclusions: The failure to perform sphincterotomy in patients with suppurative cholangitis can contribute to the backflow of bile and worse outcomes.
|
Views: 45
HTML: 2
PDF: 32
|
Background: Fournier’s gangrene represents a life-threatening necrotising infection affecting the perineal region, while hidradenitis suppurativa is characterised by a chronic inflammatory skin condition. The simultaneous occurrence of both conditions is exceedingly rare.
Case description: A 42-year-old female with a documented history of severe untreated hidradenitis suppurativa presented for shortness of breath, fever and lethargy, along with extensive wounds and skin breakdown involving the left axilla, perineum, lower back, lumbosacral region and bilateral gluteal areas, extending to the perineum. Upon presentation, the patient was in a state of septic shock, and a diagnosis of actively manifesting Fournier’s gangrene was established at the site of the pre-existing hidradenitis suppurativa lesions. Despite the implementation of an aggressive multidisciplinary approach incorporating surgical interventions, antibiotic therapy and intensive care measures, the patient’s condition deteriorated, culminating in septic shock, multi-organ failure and eventual demise. In this report, we discuss both clinical entities, their similarities and differences, and the possible mechanisms by which they may have co-occurred.
Conclusion: The co-existence of hidradenitis suppurativa and Fournier’s gangrene poses unique challenges, given the rapid progression of Fournier’s gangrene within the context of hidradenitis suppurativa, potentially suggesting the latter as a predisposing factor. This case underscores the importance of vigilant screening and management of hidradenitis suppurativa.
|
Views: 40
HTML: 3
PDF: 29
|
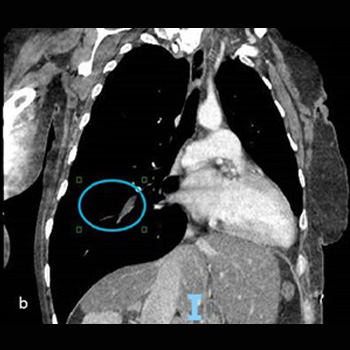
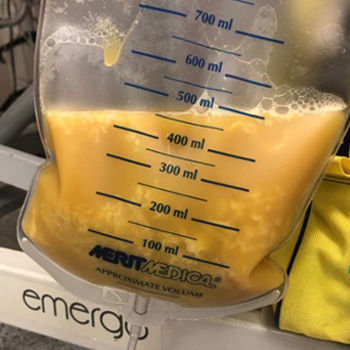
Background: Small cell lung cancer is an aggressive tumor with a poor prognosis that requires prompt treatment. While radiotherapy may enhance survival when superior vena cava syndrome is present, radiation therapy–induced pericardial disease can be a potential complication.
Case Report: A 55-year-old man, who recently underwent radiotherapy for stage IV small-cell lung cancer complicated by superior vena cava syndrome, presented with chest pain and dyspnea. In the emergency room, he was dyspneic, hypotensive, and tachycardic. Pulmonary auscultation revealed the absence of lung sounds on the right. The initial electrocardiogram showed ST-segment elevation in lateral leads and in lead DII, with reciprocal changes in lead DIII. A bedside transthoracic echocardiogram revealed cardiac tamponade and emergent pericardiocentesis was performed, removing 500 ml of purulent fluid, resulting in an immediate clinical improvement. Thoracentesis was also performed, showing no empyema. Large spectrum empirical antibiotic therapy was started. Cultures from the pericardial fluid and peripheral blood grew multi-sensitive Streptococcus pneumoniae. Cytological analysis of the pericardial fluid was consistent with infection. The patient improved after 2 weeks of targeted antibiotic therapy and underwent the first cycle of chemotherapy. He was discharged with an early scheduled pulmonology appointment.
Conclusions: Although the most common causes of pericardial effusion in lung cancer are malignant, non-malignant etiologies should also be considered. This patient had an infectious pericardial effusion most probably due to a pericardial-mediastinal mass fistula caused by radiotherapy. This was a diagnostic challenge, both in the emergency room as well in the inpatient setting.
|
Views: 51
HTML: 7
PDF: 34
|
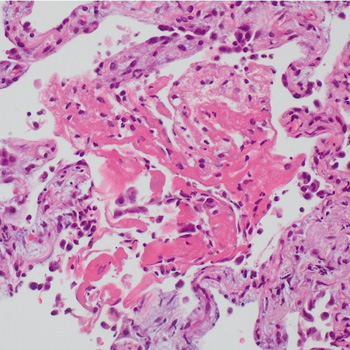
A patient initially treated with corticosteroids for cryptogenic organising pneumonia following pulmonary infarction, developed a worsening condition with progressive cavitary formations in both lower lung lobes. Contrast-enhanced chest computed tomography revealed a pulmonary embolism, and serum anti-Aspergillus IgG antibody analysis yielded a strong positive result. Consequently, the patient was diagnosed with pulmonary infarction with Aspergillus infection; organising pneumonia in surrounding areas reflected the repair process. Following treatment with anticoagulants and antifungal agents, the patient was successfully discharged. Hence, pulmonary infarction should be considered in cases of refractory lung lesions.
|
Views: 126
HTML: 9
PDF: 66
|
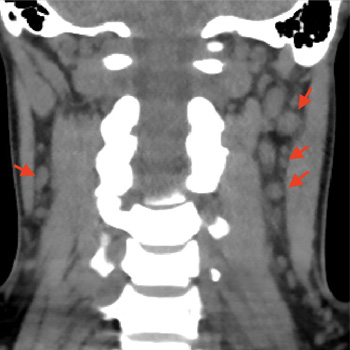
Syphilis, a disease caused by the bacteria Treponema pallidum, has a multitude of clinical manifestations and is classified into primary syphilis, secondary syphilis and tertiary syphilis, based on clinical presentations and the time elapsed since the primary infection. The secondary stage of the disease can affect multiple organs and systems, and some of these involvements may be general and non-specific, justifying its name as ‘the great imitator’. We present a case of a 30-year-old woman with a history of painful neck lymph nodes with progressive enlargement, persistent headache, weight loss, myalgia and alopecia. During investigations, stomatitis on the dorsal face of the tongue developed. A secondary study showed serum positive for rapid plasma reagin (RPR) and T. pallidum haemagglutination (TPHA), negative RPR in cerebrospinal fluid and normal MRI, thus the diagnosis of secondary syphilis was made. The patient was treated with a single dose of penicillin with complete resolution of symptoms. The case highlights the need for an exhaustive clinical examination, especially in cases presenting with non-specific and general symptoms, and raises awareness for this disease which has increased its prevalence in the last decades.
|
Views: 46
HTML: 5
PDF: 25
|
Introduction: Orthotopic heart transplantation is the gold standard for the treatment of advanced heart failure in the absence of contraindications. Infective endocarditis is a rare complication in patients after heart transplantation. The treatment of endocarditis after heart transplantation is challenging since there is a need for ongoing immunosuppression.
Case description: We present the case of a 51-year-old orthotopic heart transplant recipient enrolled in a chronic dialysis program, in whom we diagnosed and successfully treated recurrent infective endocarditis of the mitral valve caused by Enterococcus and Enterobacter species. Despite the complicated course of the disease, the treatment was successful.
Conclusions: Recurrent infective endocarditis after heart transplantation can be treated successfully with a multidisciplinary approach and robust antimicrobial therapy.
|
Views: 168
HTML: 43
PDF: 98
|
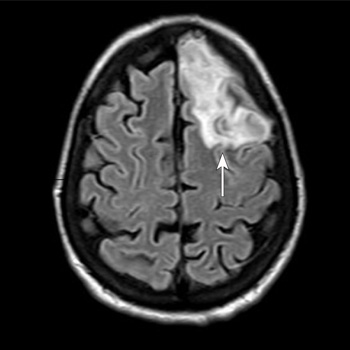
Background: Community-acquired bacterial meningitis in adults represents one of the most severe infectious diseases worldwide with potentially life-threatening medical complications. Several infectious agents can cause acute meningitis. Although group B Streptococcus is more prevalent in newborns, infection can also lead to meningitis in older adults, particularly those with underlying health issues.
Case Description: A 53-year-old woman with a body mass index of 28.7 kg/m2, type 2 diabetes mellitus, and dyslipidaemia presented to the emergency department of Santa Maria della Stella Hospital (Orvieto, Italy) with confusion, low-grade fever, echolalia, and hyperglycaemia. Computed tomography scans of the brain revealed a hypodensity in the left anterior frontal lobe and an osteodural defect of the rhinobase. Meningitis was suspected and empiric broad-spectrum antibiotic therapy with corticosteroids and insulin were administered while the results of the cerebrospinal fluid analysis confirmed the diagnosis of group B Streptococcus meningitis. Repeat imaging at 48 hours revealed enlargement of the hypodense lesion. The frontal assessment battery indicated deficits in executive functions. Prompt treatment led to rapid clinical improvement. Following the restoration of euglycemic status and hemodynamic stabilization, a follow-up magnetic resonance imaging confirmed the ischaemic lesion and showed cerebrospinal fluid in the sella turcica. The patient was then transferred to neurorehabilitation.
Conclusions: The complex interactions among multiple risk factors resulted in an atypical clinical case of group B Streptococcus meningitis, which was promptly treated with empiric antibiotic therapy to mitigate neurocognitive deficits.
| 2.1 = | 1.751 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

