EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 93
HTML: 20
PDF: 44
|
Legionella pneumophila is a bacterium that usually causes pulmonary disease but can rarely present with extrapulmonary manifestations, such as rhabdomyolysis. This is a case of Legionella infection with significant rhabdomyolysis but a lack of acute kidney injury.
A 38-year-old male with a history of epilepsy presented to the emergency department after a seizure episode with confusion, fever, emesis and bruises. He also complained of a productive cough and scant haemoptysis for the past two months. Chest X-ray showed retrocardiac and left upper lobe opacities; urine was positive for Legionella antigen and myoglobinuria. Creatinine phosphokinase was 242,488 U/l and creatinine was 0.5 mg/dl. The patient was managed with oxygen therapy, aggressive IV hydration and IV azithromycin, and later IV levofloxacin until his symptoms resolved.
Rhabdomyolysis may be a sign of Legionella infection. Rapid testing of Legionella antigen, especially in populations at risk, may be crucial for timely diagnosis and treatment. Kidney function may be preserved in the early stages of disease, but early treatment with antibiotics and aggressive hydration are an effective way to prevent deterioration in kidney function.

|
Views: 117
HTML: 13
PDF: 82
|
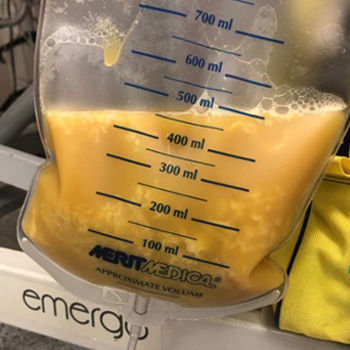
Background: Chylothorax can be classified into traumatic and nontraumatic based on the etiology. Nephrotic syndrome is a very rare cause of nontraumatic chylothorax in adults.
Case presentation: A 66-year-old woman with membranous nephropathy who was non-compliant with her management, presented with dyspnea, and was found to have a large right sided chylothorax. Her chylothorax was secondary to membranous nephropathy after excluding other causes, which has been rarely reported in literature.
Conclusion: This case highlights the possibility of nephrotic syndrome causing chylothorax, especially in patients with undiagnosed nephrotic syndrome or patients non-compliant with their management. When evaluating a patient with chylothorax, providers should consider nephrotic syndrome in the differential diagnosis.

|
Views: 176
HTML: 13
PDF: 153
|
Hamman syndrome is defined as dissection of air in mediastinum and skin fascia usually due to increased intrathoracic pressure. The air leak tends to make its way into pleural and pericardial layers; however, in rare instances air can also dissect into epidural spaces, regarded as pneumorrhachis. We present a case of a young male with a history of polysubstance abuse and e-vaping, who presented with symptoms of altered mental status. Given the concerning physical examination, a computed tomography of the chest was undertaken, which showed pneumothorax, pneumomediastinum and pneumorrhachis. The patient was closely monitored in the intensive care unit and improved after symptomatic management. The symptoms of pneumorrhachis depend on the volume and location of air in intracranial and intraspinal space. Although asymptomatic in our case, it is crucial for clinicians to be aware that pneumorrhachis with Hamman syndrome can potentially cause neurological deficits and cardiopulmonary arrest in severe cases due to increased intraspinal and intracranial hypertension, emphasising the need for close monitoring.
|
Views: 256
HTML: 20
PDF: 203
|
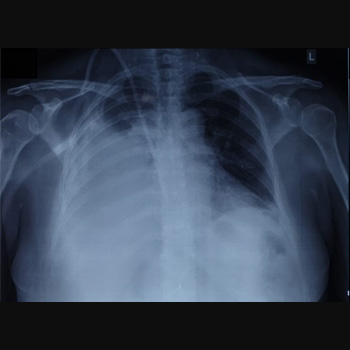
Background: Small cell lung cancer is an aggressive tumor with a poor prognosis that requires prompt treatment. While radiotherapy may enhance survival when superior vena cava syndrome is present, radiation therapy–induced pericardial disease can be a potential complication.
Case Report: A 55-year-old man, who recently underwent radiotherapy for stage IV small-cell lung cancer complicated by superior vena cava syndrome, presented with chest pain and dyspnea. In the emergency room, he was dyspneic, hypotensive, and tachycardic. Pulmonary auscultation revealed the absence of lung sounds on the right. The initial electrocardiogram showed ST-segment elevation in lateral leads and in lead DII, with reciprocal changes in lead DIII. A bedside transthoracic echocardiogram revealed cardiac tamponade and emergent pericardiocentesis was performed, removing 500 ml of purulent fluid, resulting in an immediate clinical improvement. Thoracentesis was also performed, showing no empyema. Large spectrum empirical antibiotic therapy was started. Cultures from the pericardial fluid and peripheral blood grew multi-sensitive Streptococcus pneumoniae. Cytological analysis of the pericardial fluid was consistent with infection. The patient improved after 2 weeks of targeted antibiotic therapy and underwent the first cycle of chemotherapy. He was discharged with an early scheduled pulmonology appointment.
Conclusions: Although the most common causes of pericardial effusion in lung cancer are malignant, non-malignant etiologies should also be considered. This patient had an infectious pericardial effusion most probably due to a pericardial-mediastinal mass fistula caused by radiotherapy. This was a diagnostic challenge, both in the emergency room as well in the inpatient setting.

|
Views: 266
HTML: 49
PDF: 222
|
Prostate cancer can metastasise to the lung. Most common presentations described in the literature are solitary pulmonary nodules, lymphangitic spread and, rarely, pleural effusion.
We describe a case of prostate adenocarcinoma with diffuse bilateral reticulonodular and lymphangitic pulmonary metastasis, and malignant pleural effusion while being on androgen deprivation therapy.
|
Views: 199
HTML: 17
PDF: 159
|
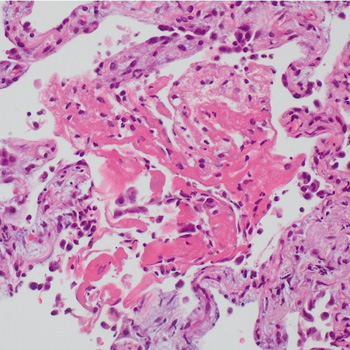
A patient initially treated with corticosteroids for cryptogenic organising pneumonia following pulmonary infarction, developed a worsening condition with progressive cavitary formations in both lower lung lobes. Contrast-enhanced chest computed tomography revealed a pulmonary embolism, and serum anti-Aspergillus IgG antibody analysis yielded a strong positive result. Consequently, the patient was diagnosed with pulmonary infarction with Aspergillus infection; organising pneumonia in surrounding areas reflected the repair process. Following treatment with anticoagulants and antifungal agents, the patient was successfully discharged. Hence, pulmonary infarction should be considered in cases of refractory lung lesions.

|
Views: 138
HTML: 16
PDF: 162
|
Lung underdevelopment is a rare congenital anomaly with variable clinical significance and presenting symptoms. It usually manifests during childhood. We present two cases of developmental lung anomaly subtypes and discuss clinical presentation and outcomes in such patient populations.
|
Views: 167
HTML: 17
PDF: 144
|
Pleuroperitoneal leak as a cause of pleural effusions in peritoneal dialysis is a rare but important complication to consider in continuous ambulatory peritoneal dialysis (CAPD) patients presenting with recurrent progressive dyspnoea. Generally, these effusions are unilateral and right-sided, resulting in shortness of breath and reduced ultrafiltration volume, which are initially managed by peritoneal rest. We describe a case of bilateral pleural effusions in a 57-year-old female on chronic CAPD who developed recurrent progressive dyspnoea but maintained adequate dialysis output. A chest radiograph revealed bilateral pleural effusions with high glucose content, and scintigraphy confirmed the existence of a definite pleuroperitoneal communication. She was managed by temporary substitution to haemodialysis, followed by suturing of the shunt and successful video-assisted thoracoscopic surgery (VATS) pleurodesis with an aldehyde-based surgical glue. Unexplained recurring dyspnoea in chronic CAPD should raise the suspicion of a possible pleuroperitoneal leak, even in patients without an apparent loss of ultrafiltration. Pleurodesis using an aldehyde-based adhesive was effective and tolerated well by our patient and may be considered in managing cases of recurrent pleural effusion.
|
Views: 217
HTML: 115
PDF: 210
|
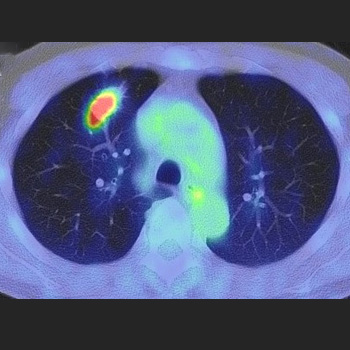
A 69-year-old man was diagnosed with lung adenocarcinoma with metastasis because two masses in the right intercostal space and right back muscle showed high accumulation on positron emission tomography (PET). The 6-month treatment with osimertinib significantly reduced his lung lesion, but no changes were observed in the metastatic lesions. Needle biopsy revealed that the lesion in the right back muscle was a schwannoma. Surgical resection revealed that the right intercostal lesion was also a schwannoma; subsequently, a right upper lobectomy was performed. The patient was finally diagnosed with lung adenocarcinoma without metastasis. High accumulations of lesions observed on PET may indicate schwannomas.

|
Views: 422
HTML: 82
PDF: 376
|
Legionnaire's disease can cause rare and severe complications such as rhabdomyolysis and acute kidney injury. This case report details a 45-year-old male patient who presented with features of Legionnaire's disease. Laboratory results showed a significantly elevated serum creatinine kinase level and an increased creatinine level. Imaging showed right lower lobe consolidation, and a positive urine antigen test confirmed Legionnaire's disease. The patient was administered azithromycin and underwent fluid repletion to manage the rhabdomyolysis and acute kidney injury, resulting in improved creatinine kinase levels and kidney function. He was discharged and continued on azithromycin for 10 days. His outpatient follow-up showed that creatinine kinase levels had further decreased. This case report emphasises the importance of early recognition and management of Legionnaire's disease and its rare but severe complications.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

