EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 337
HTML: 68
PDF: 212
|
The incidence of post-infectious autoimmune diseases has been on the rise following the COVID-19 pandemic. Recently, an autistic patient was admitted to the hospital presenting with a mild upper respiratory system COVID-19 infection. Months after recovery and polymerase chain reaction negativity, the patient developed HEp-2 cell positivity and presented with relapsing polychondritis (RP), a rare autoimmune disease. The mechanism of this autoimmune invasion is ultimately caused by activating a myriad of immune reactions. Lymphocytopenia almost always accompanies various clinical forms of COVID-19; however, it may drive the lymphocytopenia-induced proliferation of autoreactive T cells via the activation of interleukin-6 (IL-6). Moreover, high levels of neutrophils during infection promote autoimmune disease by releasing cytokine and chemokine cascades that accompany inflammation, and neutrophil extracellular traps regulating immune responses through cell–cell interactions. Furthermore, autism spectrum disorder patients display an altered immune system that includes an augmented inflammatory cytokine milieu leading to an increased pro-inflammatory Th1/Th2 ratio. In addition, the pathophysiology of RP is majorly associated with a cell-mediated immune reaction; thus, the predisposing exaggerated immune system of such patients must also be considered as a predisposing factor to the development of post-infectious autoimmune diseases.

|
Views: 437
HTML: 24
PDF: 201
|
Background: Vaccine-induced immune thrombotic thrombocytopenia (VITT) is a rare life-threatening thrombotic reaction to COVID-19 vaccines.
Case description: Two young male first cousins, with a family history of idiopathic thrombocytopenic purpura, developed VITT after the Ad26.COV2.S vaccine. Both had a favourable clinical and analytical outcome. We investigated the genetic factors that could be associated with a genetic predisposition to VITT.
Conclusions: There are no published cases where the VITT patients were relatives. The genetic study did not reveal any likely pathogenic variants, although the prevalent polymorphism c.497A>G (p.(His166Arg)) in the FCGR2A gene was found in a homozygous state. More studies are required to better understand VITT’s pathophysiology and any underlying genetic predispositions.
|
Views: 563
HTML: 39
PDF: 311
|
Background: Although there is no specific therapy for COVID-19, it is recommended that patients with severe SARS-CoV-2 infection are treated with corticosteroids and anti-IL-6 receptor monoclonal antibodies. Both COVID-19 itself and the treatment modalities mentioned above have suppressive effects on the immune system which may lead to an increased susceptibility to other infections. In patients with latent tuberculosis (TB) reactivation of TB infection after recovery from severe COVID-19 has been described. Most of these cases have occurred in parts of the world where tuberculosis is endemic.
Case description: The patient is a female in her 70s who was born and raised in Southeast Asia and has lived in the Netherlands for more than 30 years. She was treated for a severe COVID-19 requiring mechanical ventilation for several weeks and pharmaceutical treatment with corticosteroids and anti-IL-6 receptor monoclonal antibodies (Sarilumab). She recovered well. Two years later she was readmitted with symptoms of a serious pulmonary infection and meningitis. Her condition deteriorated in a short time. An active TB infection was diagnosed. Despite adequate antibiotic treatment and supportive therapy her condition worsened and four days after admission to the ICU she deceased.
Discussion: Reactivation of latent TB after recovery from a severe COVID-19 has been described several times and may occur several months after the SARS-CoV-2 infection. In this case the reactivation presented two years after COVID-19. This case illustrates that long-term follow-up of patients with latent TB that recover from a severe COVID-19 may be indicated.
|
Views: 355
HTML: 18
PDF: 244
|
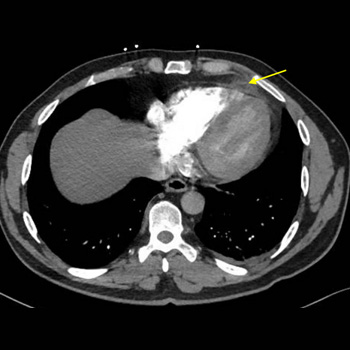
Background: Epipericardial fat necrosis (EFN) is a rare and self-limiting cause of acute chest pain. We describe a case of EFN in a patient with a recent coronavirus disease (COVID-19).
Case Presentation: A 55-year-old male presented with a sudden onset of left-sided pleuritic chest pain for the past two days. The patient was diaphoretic, tachypneic, and tachycardic. Acute coronary syndrome was ruled out. A computed tomography (CT) pulmonary angiogram revealed an ovoid encapsulated fatty mass surrounded by dense appearing tissue. Patient symptoms improved remarkably with a short course of non-steroidal anti-inflammatory drugs (NSAIDs).
Discussion: EFN typically presents with a sudden onset of excruciating chest pain. Misdiagnosis, under-diagnosis, and mismanagement are unavoidable. EFN is incidentally diagnosed on CT scan. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infects visceral adipose tissue and appears to increase the risk of EFN by promoting inflammatory cytokine production and death of adipocytes.
Conclusion: EFN is a rare cause of acute chest pain. SARS-CoV-2 is likely to induce EFN. This rare clinical entity should be considered in the differential of acute chest pain especially in patients with active or recent COVID-19.
|
Views: 353
HTML: 25
PDF: 278
|
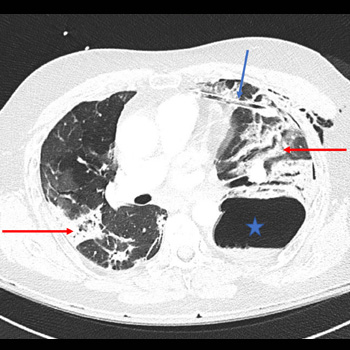
Background: Until now, only a few cases of Valsalva-induced barotraumas (pneumothorax, pneumomediastinum and subcutaneous emphysema) have been described, and none of them among COVID-19 patients.
Case description: A man in his 50s was admitted for SARS-CoV-2-related acute respiratory distress syndrome (ARDS). Initial evolution was favourable with non-invasive ventilatory support, high-flow oxygen nasal cannula and the best supportive drugs available at the time. During the Valsalva manoeuvre while defecating, the patient reported sudden chest pain and showed a new acute hypoxemic respiratory failure due to a pneumothorax. It led to multiple complications (pulmonary embolism, haemoptysis, and cardiac arrest), and despite the best supportive care, led to the patient's death.
Discussion: The Valsalva manoeuvre can be an overlooked cause of pneumothorax in patients with COVID-19. Predisposition to barotrauma in COVID-19 patients could be explained by several factors, including the extensive use of non-invasive and invasive ventilation during the pandemic, and the histological changes observed in the lungs of those infected with COVID-19.
Conclusion: We report the first description of a Valsalva-induced barotrauma in a COVID-19 infection. We emphasise the importance of treating constipation particularly in severe COVID-19 cases, to prevent complications such as barotrauma.
|
Views: 272
HTML: 45
PDF: 216
|
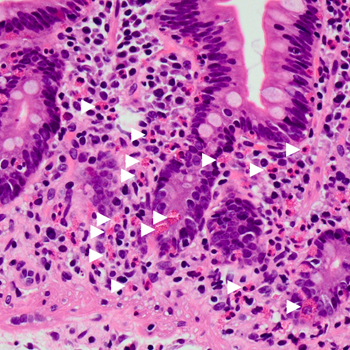
Introduction: Large-scale clinical studies for COVID-19 vaccines have shown the infection-preventing effect and short-term adverse effects. Some rare illnesses such as eosinophilia can develop following COVID-19 vaccinations.
Case description: We report a case of 65-year-old man with unexplained abdominal pain that developed 2 weeks after COVID-19 mRNA vaccination. The patient had received a second dose of COVID-19 mRNA vaccine and revealed eosinophilia at the first visit to our hospital. Eosinophil infiltration was observed in the lamina propria of the duodenum by a step biopsy. Montelukast 10 mg was administered as the initial treatment of eosinophilic gastroenteritis (EGE), and the abdominal pain was improved.
Discussion: The strong influence of COVID-19 vaccination on the development of EGE remains unproven. Reports of eosinophilia following COVID-19 vaccination have discussed that COVID-19 mRNA vaccination triggered an eosinophilic response.
Conclusion: This case presented EGE that developed following COVID-19 mRNA vaccination, which would be a rare adverse event.

|
Views: 369
HTML: 33
PDF: 293
|
Introduction: We present a case of anion gap euglycemic diabetic ketoacidosis (EuDKA) in a patient with COVID-19 infection. Patients with diabetes mellitus are at increased risk of severe illness, and hyperglycaemia is associated with higher morbidity and mortality in patients infected with COVID-19.
Case Description: A 76-year-old male with diabetes mellitus treated with SGLT2 inhibitor tested positive for COVID-19 infection on day 3 after his admission. In the emergency room he had a high anion gap metabolic acidosis and a blood glucose of 248 mg/dl. His urine tested strongly positive for ketones. A diagnosis of euglycemic diabetic ketoacidosis was made and he was treated with intravenous insulin and normal saline; his antidiabetic medications were stopped. His metabolic acidosis gradually resolved, and he was discharged.
Discussion: Euglycemic diabetic ketoacidosis is a rare complication of COVID-19 infection. It is defined by the American Diabetes Association as the triad of anion gap metabolic acidosis with arterial pH <7.3, serum bicarbonate <18 mmol/l and ketonuria or ketonemia. It is a life-threatening complication which usually occurs in type 1 diabetes mellitus patients but may also occur in type 2 diabetes mellitus patients. As described earlier, it is associated with hyperglycaemia but if blood glucose is low or near normal but <250 mg/dl it is then named euglycemic diabetic ketoacidosis. Patients treated with SGLT2 inhibitors are at increased risk of euglycemic diabetic ketoacidosis.
Conclusions: COVID-19 infection precipitated euglycemic diabetic ketoacidosis in our patient. SGLT2 inhibitors must be stopped when this adverse reaction occurs. As their use increases, the risk of this adverse reaction is higher as well. Their prescription should be restricted to trained physicians who are able to educate their patients and treat them appropriately in situations that may arise.

|
Views: 212
HTML: 52
PDF: 219
|

|
Views: 413
HTML: 113
PDF: 283
|
Background: Beau's lines are transverse grooves in the nail plate that result from transient interruption of the growth of the proximal nail matrix. These rare nail disorders can be triggered mostly by infections or systemic diseases.
Case Description: We describe a 65-year-old man who presented with nail changes on all fingernails. The patient, a non-smoker with no medication history, had severe immune responses during two hospitalisations, 9 and 4 months ago, for COVID-19. Both hospitalisations were accompanied by markedly elevated interleukin-6 levels, and treatment with tocilizumab on top of dexamethasone was required. The present examination revealed Beau's lines which were associated with both prior COVID-19 infections.
Conclusions: Although nail changes look harmless, seeking Beau's lines during the physical examination might indicate past severe COVID-19 infection and a higher probability for reinfection and rehospitalisation.

|
Views: 345
HTML: 67
PDF: 275
|
Introduction: Individuals who have had severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection may develop post-coronavirus disease conditions, also known as long COVID. The symptoms of long COVID are nonspecific, and there are similarities between the symptoms of long COVID and those of Graves’ disease (GD). Therefore, it is important to rule out GD in patients suspected of having long COVID. Telemedicine is widely used to avoid the risk of SARS-CoV-2 infection. However, owing to the lack of in-person examinations, diagnostic errors can occur.
Case description: A 27-year-old Japanese woman presented complaining of persistent fatigue, dyspnea, and low-grade fever, and after in-person examination was finally diagnosed with GD. She had been diagnosed with SARS-CoV-2 infection four months earlier and her symptoms had resolved within 5 days but then recurred. Subsequently, she had 3 telemedicine visits and had been diagnosed with long COVID.
Discussion: With telemedicine there may be delayed diagnosis of GD in patients with a recent history of SARS-CoV-2 infection. Some symptoms and abnormalities cannot be confirmed in telemedicine visits performed using a simple mobile phone. Therefore it is important to know which findings obtained in telemedicine visits with a simple mobile phone are suggestive of GD. Low-grade fever and tachycardia are often observed in patients with GD, but rarely occur in patients with long COVID.
Conclusion: Tachycardia and persistent low-grade fever after SARS-CoV-2 infection, which can be confirmed by telemedicine, can be clues for the diagnosis of GD. Therefore, in-person examination should be added if these symptoms are confirmed by telemedicine.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

