EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 266
HTML: 37
PDF: 170
|
Addison’s disease is a rare, autoimmune condition leading to the destruction of the adrenal gland. Autoimmune conditions are known to commonly co-occur. When Addison’s disease presents in the setting of autoimmune thyroid disease and/or type 1 diabetes, this condition is termed autoimmune polyendocrine syndrome type II, a rare endocrinopathy found in roughly 1.4-4.5 per 100,000 individuals. Here, we describe a clinical case presenting with hypotension refractory to fluid resuscitation and electrolyte derangements later diagnosed as autoimmune polyendocrine syndrome type II.

|
Views: 476
HTML: 26
PDF: 313
|
Euglycemic diabetic ketoacidosis (euDKA) is a rare but severe metabolic complication of diabetes mellitus characterised by elevated anion gap metabolic acidosis despite normal or mildly elevated blood glucose levels. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have emerged as effective antidiabetic medications, yet their use is associated with an increased risk of euDKA, especially when coupled with insulin dose reduction.
We present the case of a 50-year-old male with a 20-year history of diabetes mellitus, initially managed with insulin and metformin, who developed euDKA following the introduction of empagliflozin and sitagliptin alongside a reduction in insulin therapy. Despite normoglycaemia the patient exhibited symptoms of ketoacidosis, including chronic fatigue, polydipsia, and polyuria.
Diagnostic workup revealed metabolic acidosis, elevated inflammatory markers, acute kidney injury and ketonuria. Subsequent specialised laboratory tests confirmed type 1 diabetes mellitus (T1DM) with the presence of anti-glutamic acid decarboxylase (anti-GAD) antibodies and the absence of C-peptide secretion. Management involved fluid therapy, intravenous insulin and glucose administration.
This case underscores the diagnostic challenges of euDKA and emphasises the importance of differentiating between T1DM and T2DM, as management strategies vary significantly. Patient education on insulin therapy and injection techniques is crucial to prevent complications such as improper insulin delivery and dose reduction, which can precipitate euDKA.
In conclusion, clinicians should be vigilant for euDKA in patients on SGLT2 inhibitors, particularly when insulin dose reduction is involved. Comprehensive patient education and accurate differentiation between diabetes types are essential for timely diagnosis and optimal management, thereby reducing the risk of severe complications.
|
Views: 320
HTML: 56
PDF: 231
|
Background: Community-acquired bacterial meningitis in adults represents one of the most severe infectious diseases worldwide with potentially life-threatening medical complications. Several infectious agents can cause acute meningitis. Although group B Streptococcus is more prevalent in newborns, infection can also lead to meningitis in older adults, particularly those with underlying health issues.
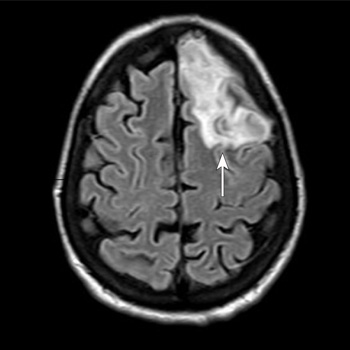
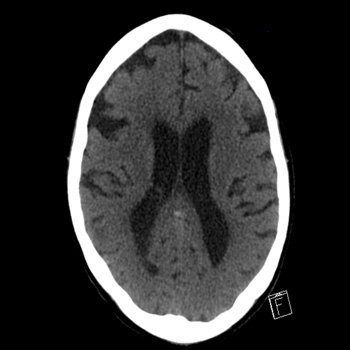
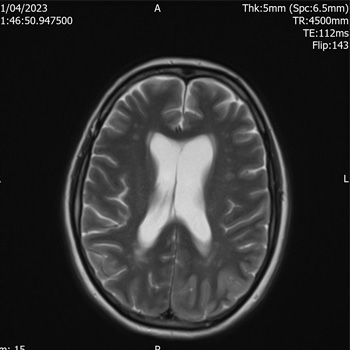
Case Description: A 53-year-old woman with a body mass index of 28.7 kg/m2, type 2 diabetes mellitus, and dyslipidaemia presented to the emergency department of Santa Maria della Stella Hospital (Orvieto, Italy) with confusion, low-grade fever, echolalia, and hyperglycaemia. Computed tomography scans of the brain revealed a hypodensity in the left anterior frontal lobe and an osteodural defect of the rhinobase. Meningitis was suspected and empiric broad-spectrum antibiotic therapy with corticosteroids and insulin were administered while the results of the cerebrospinal fluid analysis confirmed the diagnosis of group B Streptococcus meningitis. Repeat imaging at 48 hours revealed enlargement of the hypodense lesion. The frontal assessment battery indicated deficits in executive functions. Prompt treatment led to rapid clinical improvement. Following the restoration of euglycemic status and hemodynamic stabilization, a follow-up magnetic resonance imaging confirmed the ischaemic lesion and showed cerebrospinal fluid in the sella turcica. The patient was then transferred to neurorehabilitation.
Conclusions: The complex interactions among multiple risk factors resulted in an atypical clinical case of group B Streptococcus meningitis, which was promptly treated with empiric antibiotic therapy to mitigate neurocognitive deficits.

|
Views: 414
PDF: 319
HTML: 150
|
Marijuana has long been used both for recreational and medicinal purposes. Most of the available forms of marijuana contain additives such as liquorice to enhance its flavour. Liquorice increases the amounts of cortisol in the body and produces metabolic abnormalities seen in primary hyperaldosteronism. Liquorice extracts are mixed with marijuana in the same way as for tobacco. We describe a case of apparent mineralocorticoid excess due to excessive smoking of liquorice-laced marijuana. To our knowledge, this is the first reported case of apparent mineralocorticoid excess caused by marijuana use.
|
Views: 494
HTML: 58
PDF: 461
|
We present a case of thyrotoxic periodic paralysis (TPP) presenting with stroke symptoms as a harbinger of Grave’s disease. A 61-year-old female presented with symptoms of abdominal pain and fatigue two weeks prior to admission and reported acute diarrhoea and unintentional weight loss. Investigation revealed thyrotoxicosis with undetectable thyroid stimulating hormone (TSH), elevated free T4 and elevated thyroid stimulating immunoglobulin (TSI). On the third day of admission, while undergoing physical therapy, code stroke was called on account of the onset of right-side predominant acute flaccid paralysis of upper and lower extremities, right-side facial droop, dysarthria and hyporeflexia bilaterally. The patient was alert and fully oriented with stable vitals with no increased labour in breathing at room air. An emergent head and neck CT, angiography, and magnetic resonance imaging (MRI) were negative. Serum potassium was 2.7 mmol/l, requiring prompt replacement. The patient’s paralysis and dysarthria improved over the following three days with a complete reversal of symptoms following the correction of serum potassium. Thyrotoxic periodic paralysis can occur in association with any of the causes of hyperthyroidism. It is due to a significant intracellular shift of potassium, subsequently manifesting clinically with hypokalaemia and muscle paralysis.
|
Views: 364
HTML: 51
PDF: 326
|
Introduction: Visual seizure is one of the rare complications of poorly controlled chronic hyperglycaemia. This condition can be debilitating for patients. Early recognition and careful control of hyperglycaemia is vital.
Case description: A middle-aged female was found collapsed at her home after missing insulin for several days. She was found to have diabetes ketoacidosis (DKA) and she was started on treatment for DKA. She reported visual hallucinations in the right side of her visual field for a week. Further assessment with EEG and brain MRI suggested an occipital seizure consistent with metabolic disturbances. She was initially started on antiepileptic medication. After strict diabetes control, her symptoms resolved, and she no longer needed antiepileptic treatment.
Conclusion: Experiencing diabetes-related seizures can be terrifying both for patients and their family. Early recognition and quick control of hyperglycaemia is important in treating these patients.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

