EJCRIM 2023 CiteScore
| 2.1 = | 1.751 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by




|
Views: 23
HTML: 3
PDF: 10
|
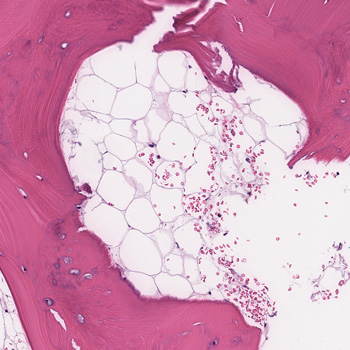
Background: Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease, characterised by multi-organ affections. Haematological involvement is a common manifestation of SLE, consisting of autoimmune peripheral cytopenia. Autoimmune myelofibrosis (AIMF) is a rare cause of cytopenia in SLE; it could precede or be concurrent with the diagnosis of SLE. There are few studies that describe this association.
Case description: We report a case of AIMF revealing the diagnosis of SLE in a 34-year-old female, presented with episodes of gingival bleeding associated with peripheral inflammatory polyarthralgia, photosensitivity and deterioration of general condition. Clinical examination revealed a soft pitting oedema in the lower limbs. Laboratory investigations showed a pancytopenia, inflammatory biological syndrome, with positive 24-hour proteinuria and anti-native DNA antibodies. A bone marrow biopsy showed diffuse myelofibrosis associated with maturation disorders and no tumour infiltrate. Renal biopsy revealed proliferative glomerulonephritis class III with immune deposits.
Conclusion: The association of AIMF with SLE has been rarely reported, and it could be another cause for cytopenia in SLE.

|
Views: 58
HTML: 4
PDF: 23
|
Introduction: Blue rubber bleb nevus syndrome is a rare disorder of venous malformations, with around 200 cases reported. We present a case of Mycobacterium xenopi infection in a patient with blue rubber bleb nevus syndrome.
Case Description: A 40-year-old female with blue rubber bleb nevus syndrome, asthma, and bronchiectasis came to the pulmonology clinic with shortness of breath and a cough. She was recently admitted for a bronchiectasis exacerbation but continued to have a worsening productive cough and fevers. The most recent CT scan of the chest showed interval stable right upper lobe fibrocavitary disease, demonstrating gradual progression over two years. She had occasional positive cultures for Mycobacterium Avium Complex and M. xenopi one year previously, assumed to be a colonizer and not treated. Most recent hospital cultures were negative for bacteria and an acid-fast bacilli smear. She was sent to the emergency department for bronchiectasis exacerbation and returned to the clinic six weeks later with two sputum cultures growing M. xenopi. It was decided to treat M. xenopi as this was likely the cause of her cavitary lung lesion and frequent infections. Azithromycin, rifampin, and sulfamethoxazole/trimethoprim were initiated. Intravenous amikacin was added later on. She finally had a right partial lung resection done after one year at an outside hospital. She was on and off antibiotics for M. xenopi for approximately three years with negative repeat cultures for non-tuberculous mycobacteria.
Conclusion: Due to the high mortality of M. xenopi infections (which can be as high as 69%), treatment of at least twelve months is recommended. To our knowledge, this is the first reported case of M. xenopi in a patient with blue rubber bleb nevus syndrome.
|
Views: 184
HTML: 15
PDF: 86
|
Background: Melioidosis is an infection caused by Burkholderia pseudomallei, a Gram-negative bacterium. It is a disease endemic to Southeast Asia and northern Australia although its global incidence has been rising. It most commonly infects people with certain identified risk factors such as diabetes, alcoholism, thalassemia, and underlying chronic disease involving lungs, kidney and liver. This bacterium is capable of producing a wide array of clinical manifestations ranging from asymptomatic disease to localised infections such as in the lung, bone or skin to disseminated infection.
Case description: This is a case, from United Arab Emirates, of a 40-year-old male recently diagnosed with diabetes who presented with multiple abscesses and was eventually diagnosed with disseminated melioidosis. He was treated successfully with antibiotics and drainage of abscesses.
Conclusion: In non-endemic regions, melioidosis can be easily missed in common diagnostic approaches. This gap of awareness could delay the diagnosis and allow further deterioration of the patient due to complications. Thus, case reports like this can enlighten internists about changing incidences and complexity of clinical presentations, thus preparing them to better handle such patients in the future.

|
Views: 77
HTML: 5
PDF: 72
|
Background: Annular erythema is a rare manifestation of leukocytoclastic vasculitis. It may be associated with various drugs, infections, malignancies, or systemic diseases.
Case description: A 36-year-old woman with no personal medical history presented with annular erythema with target lesions and petechial purpura. The patient had fever and joint arthralgia. A skin biopsy showed leukocytoclastic vasculitis with IgA deposits on direct immunofluorescence. The diagnosis of immunoglobulin A vasculitis with annular leukocytoclastic vasculitis was made. The patient showed global improvement with topical steroids without relapse.
Conclusion: An annular variant of leukocytoclastic vasculitis is a rare manifestation of immunoglobulin A vasculitis.

|
Views: 68
HTML: 8
PDF: 65
|
Lung underdevelopment is a rare congenital anomaly with variable clinical significance and presenting symptoms. It usually manifests during childhood. We present two cases of developmental lung anomaly subtypes and discuss clinical presentation and outcomes in such patient populations.
|
Views: 219
HTML: 17
PDF: 84
|
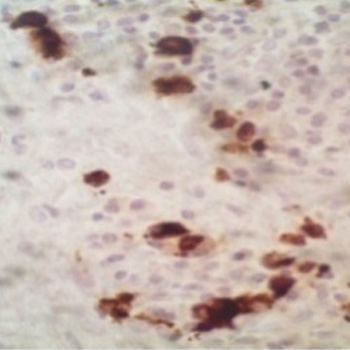
We report a rare yet successful utilisation of anti-CD20 therapy using rituximab for treatment of a case of IgG4-related mastitis proven by clinical, serological, and histopathological evidence. This was affecting a mid-aged female who was referred to the rheumatology clinic by the breast surgeons to help assessing for the possibility of an underlying inflammatory process involving the breast tissue unilaterally.
The clinical course was apparently complex with an onset of an induration in the right lateral superior quadrant of the breast with mild discomfort and heaviness sensation. This increased over a course of 2 weeks before presentation to the general surgery clinic.
Subsequent investigations confirmed that the case was IgG4-related mastitis and a trial of steroids and disease modifying anti-rheumatic drugs (DMARDs) was partially helpful, but not to a full degree, mandating the utilisation of a more advanced mode of therapy, so rituximab was selected.
|
Views: 302
HTML: 20
PDF: 176
|
Background: Autoimmune diseases are not contraindications for immune checkpoint inhibitors (ICI) therapy in patients with cancer. However, immune-related adverse events (irAEs) are frequently observed in patients receiving ICIs including dermatitis, thyroiditis, colitis, and pneumonitis. Thrombocytopenic purpura, aplasia, and haemophagocytic lymphohistiocytosis (HLH) are rarely observed during ICIs.
Case description: We report the case of a male patient with pre-existing untreated HLA B27 and ankylosing spondylitis with gastric cancer and liver metastases. The 79-year-old man was treated with anti-HER2 trastuzumab and anti-PD-1 nivolumab. Seventeen days after the seventh cycle of treatment, he presented at the emergency department with acute fever, confusion, and hypotension. Laboratory results showed pancytopenia, and elevation of ferritin and triglyceride. No infections were detected. Although not seen in a bone marrow biopsy, clinical presentation, and absence of infection, together with an H-score of 263, indicated HLH. The patient was treated with dexamethasone for four days and discharged on a tapering dose of steroids. At the two-month follow-up, clinical presentation was normal and blood test almost normalised. At 8 months, no liver metastases were observed.
Conclusions: In a patient with a pre-existing autoimmune condition, immunotherapy led to the development of HLH, which was controlled by glucocorticoid. Absence of the feature of haemophagocytosis in the bone marrow biopsy did not exclude the diagnosis, as HLH can occur in the spleen or in the liver. Glucocorticoid therapy did not prevent the anti-cancer effect of ICIs, and liver metastases disappeared 8 months post-HLH. This case warrants further research on the interplay between autoimmunity and ICI response, as well as ICI-induced irAEs.
|
Views: 146
HTML: 6
PDF: 104
|
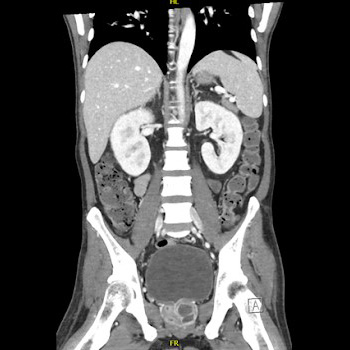
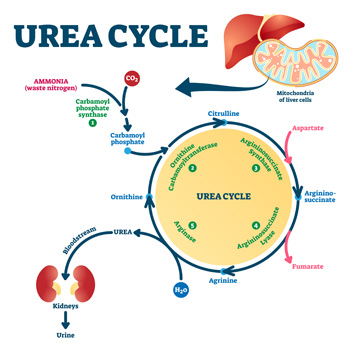
Background: Hyperargininemia is a rare inherited metabolic disorder of the urea cycle with an autosomal recessive transmission. It occurs due to a deficiency of the enzyme arginase I and causes progressive neurological damage. Very few cases are diagnosed in adulthood, with the majority being diagnosed before the age of 4. Currently, this condition is diagnosed by a mass spectrometry technique in neonatal screening, which has been implemented in Portugal since 2007; births before that were not screened for this entity.
Case description: We present a case of a 23-year-old woman referred to the internal medicine and neurology departments with a history of two hospital admissions for rhabdomyolysis at the age of 18, consanguineous parents, learning difficulties and multiple falls since the age of 8. In addition, the patient also had behavioural changes so she had psychological counselling at school, but lacked family support. Neurological examination showed mild proximal paraparesis, and spastic and paraparetic gait. The aetiological study revealed a pathological variant in homozygosity ARG1 and increased blood levels of arginine. Therefore, the diagnosis of hyperargininemia was confirmed.
Conclusions: Compared to other urea cycle disorders, hyperargininemia is the rarest one. It is important to recognise the characteristic clinical features and diagnose it early because a favourable outcome can be achieved with appropriate treatment. This case shows a delayed diagnosis of hyperargininemia and highlights the importance of the internist’s role in diagnosing rare diseases.

|
Views: 127
HTML: 14
PDF: 80
|
Background: Patients with neurofibromatosis type I (NF1) have an increased risk of developing soft-tissue sarcomas, particularly those related to the nervous system. Epithelioid sarcoma (ES) is an exceptionally rare subtype of soft-tissue sarcoma, with limited knowledge about its clinical presentation and optimal management in NF1. This report aims to provide insights into the characteristics and outcomes of ES in NF1 patients.
Case description: A 37-year-old man with a history of NF1 presented with a progressively worsening mass on his right inner thigh. An MRI scan revealed a well-defined tissue mass originating from the adductor magnus muscle, later confirmed as ES through histopathology and immunohistochemistry. Considering poor local and general prognosis, the multidisciplinary team recommended salvage hip disarticulation, however the patient refused and opted for palliative marginal resection to reduce the tumour size. The patient’s condition declined rapidly, and he succumbed six days after the surgery.
Conclusion: This case highlights the rarity of ES in NF1 patients and underscores the potential for malignant tumour development in this population. Further research is needed to improve our understanding and management of sarcomas in the context of NF1.
|
Views: 190
HTML: 41
PDF: 149
|
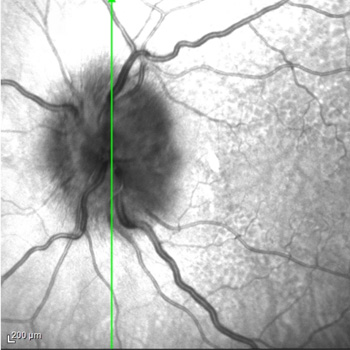
Background: eosinophilic granulomatosis with polyangiitis (EGPA) is a rare multisystem inflammatory disease characterized by asthma, eosinophilia and granulomatous or vasculitic involvement of various organs. While the eye is uncommonly affected in patients with EGPA, multiple ophthalmic manifestations have been reported, which can result in serious visual impairment without timely treatment.
Case report: we report the case of a 79-year-old woman with a history of asthma and nasal polyps who presented with low-grade fever, mild alteration of mental status, and fatigue. Chest X-ray revealed bilateral interstitial infiltrates. Lab tests showed elevated C-reactive protein level and eosinophilia (eosinophil count, 4.6 x109 cells/l); blood cultures and parasitological examination of stools tested negative. Four days after presentation, the patient reported sudden and severe blurring of vision in her left eye. Ophthalmological examination revealed bilateral swollen optic disc and visual field loss, more severe in the left eye. A diagnosis of EGPA complicated by arteritic anterior ischaemic optic neuropathy (A-AION) was proposed, while an alternative or concurrent diagnosis of giant cell arteritis was ruled out based on clinical picture.
Immunosuppressive treatment with high-dose intravenous glucocorticoids was promptly started. The patient’s visual defect did not improve; however, two months later, no worsening was registered on ophthalmic reassessment.
Conclusions: A-AION is an infrequent but severe manifestation of EGPA, requiring prompt diagnosis and emergency-level glucocorticoid therapy to prevent any further vision loss. Disease awareness and a multidisciplinary approach are crucial to expedite diagnostic work-up and effective management of EGPA-related ocular complications.
| 2.1 = | 1.751 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

