EJCRIM 2023 CiteScore
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 65
HTML: 6
PDF: 32
|
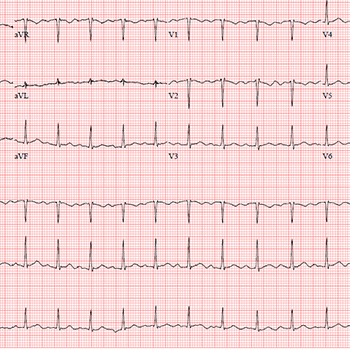
Mitral valve prolapse (MVP) is a primary valvular disease of the mitral valve with a prevalence of 2.4% of the general population. Valve abnormalities range from simple fibroelastic deficiency of the leaflets to diffuse myxomatous degenerative changes. MVP is a usually a benign condition. However, the scattered reports of sudden cardiac death in patients with MVP in the absence of severe mitral insufficiency or coronary artery disease suggest the existence of a malignant phenotype of MVP. We report a case of a young female who survived life-threatening arrhythmias and cardiac arrest and was found to have characteristic features of the malignant phenotype of MVP and had an implantable cardioverter defibrillator as a secondary prevention.

|
Views: 677
HTML: 102
PDF: 301
|
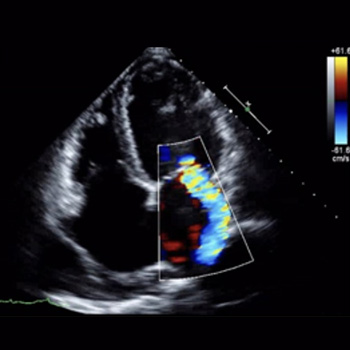
Left ventricular thrombus (LVT) formation is a serious clinical complication of low-flow states that may be seen in an ischaemic, arrhythmic heart. While LVT formation has a poor prognosis, in the setting of myocardial infarction it is usually a result of post-infarct sequelae such as left ventricle aneurysms, and inflammatory changes from damaged tissue, with the LVT taking several days to form. Arrythmias such as ventricular tachycardia (VT) or ventricular fibrillation (VF) may also lead to thrombus formation, as they contribute to stasis due to decreased cardiac output. Large anterolateral myocardial infarctions can cause electrical or arrhythmic storm, characterized by more than three episodes of VT or VF in a 24-hour period. This prolonged state of dyskinesis further increases the risk of thrombosis, creating a compounding effect. Here, we report the case of a patient who had a VF cardiac arrest with electrical storm secondary to anterolateral myocardial infarction complicated with LVT formation found on echocardiogram after the cardiac arrest, which was absent on presentation. This thrombus formation occurred particularly early during the course of the patient’s arrest, possibly due to the compounding factors increasing the risk of thrombosis. Herein, we discuss in detail the risk factors for LVT formation, its mechanism and management options. A review of the literature also shows that LVT formation in the acute phase of arrest, as seen in our patient, is rare.
|
Views: 47
HTML: 4
PDF: 23
|
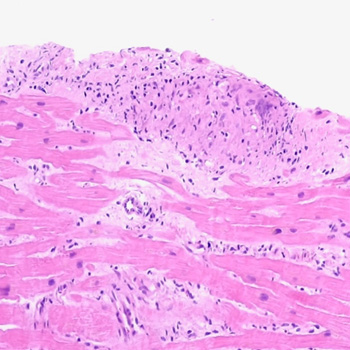
Introduction: Sarcoidosis has many possible clinical presentations since it can affect any organ, most commonly the lungs. The hallmark of the disease consists of the formation of non-necrotising granulomas. Pathogenesis is thought to rely on the interplay of genetic, environmental and epigenetic factors. This case highlights the importance of a thorough clinical history and physical examination, and the correlation with imaging findings in the diagnostic work-up of the non-ischaemic cardiomyopathy.
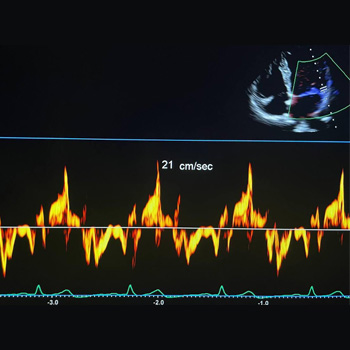
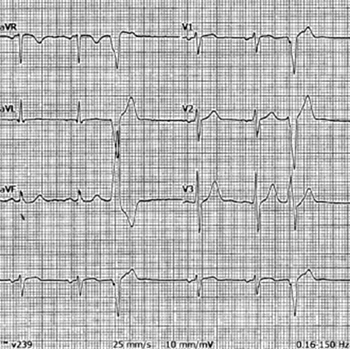
Case description: A 57-year-old woman was admitted due to the sudden onset of malaise, dizziness, and chest discomfort. Sustained monomorphic ventricular tachycardia was evidenced and the patient rapidly evolved with haemodynamic instability; she underwent successful electrical cardioversion. The electrocardiogram afterwards showed a high-risk electrocardiographic pattern. Invasive coronary angiography excluded obstructive epicardial coronary lesions. Physical examination revealed skin lesions on the lower limbs which raised suspicion for erythema nodosum and therefore a biopsy was performed. Transthoracic echocardiography and cardiac magnetic resonance imaging revealed features consistent with an inflammatory cardiomyopathy, and an implantable cardioverter-defibrillator was placed. The histologic examination of the cutaneous lesions showed a non-necrotising granulomatous inflammatory process. Radionuclide imaging was inconclusive. The patient underwent an endomyocardial biopsy, which confirmed the diagnosis of systemic sarcoidosis with cardiac involvement.
Conclusions: Systemic sarcoidosis with cardiac involvement is a challenging diagnosis. The role of imaging techniques such as transthoracic echocardiography, cardiac magnetic resonance imaging and radionuclide imaging is essential in raising suspicion and diagnosing this pathology. Endomyocardial biopsy is the ‘gold standard’ for its diagnosis; however, it has a low diagnostic yield.
|
Views: 498
PDF: 398
HTML: 81
|
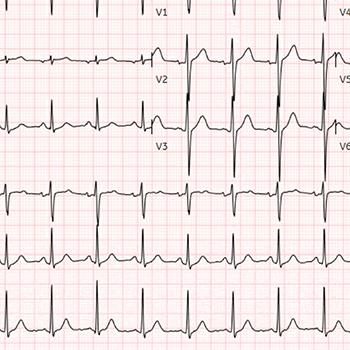
Coronavirus 19 (COVID-19) is well known for causing acute respiratory distress syndrome. Among other systemic complications, myocarditis is a frequently reported presentation as well as complication. One systematic review reported a 14% mortality rate in patients with COVID-19 myocarditis. Endomyocardial biopsy is a definitive diagnostic test but has been a challenge to perform in most cases of COVID myocarditis due to the contagious nature of the disease. Patients presenting with new cardiomyopathy with troponin leak and arrhythmias, supported by recent COVID-19 diagnosis should be suspected for COVID-induced myocarditis. Supportive treatment has been the mainstay of treatment with limited data on immunotherapy and colchicine. Our case is about a male in his 50s who had a cardiac arrest due to ventricular fibrillations, with a positive COVID-19 test. Further workup showed severe non-ischaemic cardiomyopathy with an EF of 15–20%. He was treated with intravenous immunotherapy and colchicine. A repeat echocardiogram 3 days later showed resolution of cardiomyopathy. Our case report highlights the possible beneficial effects of immunotherapy and colchicine in viral myocarditis.
|
Views: 69
HTML: 7
PDF: 43
|
Background: This study presents a patient diagnosed with tricuspid valvular stenosis due to right ventricular lymphoma, who was treated successfully.
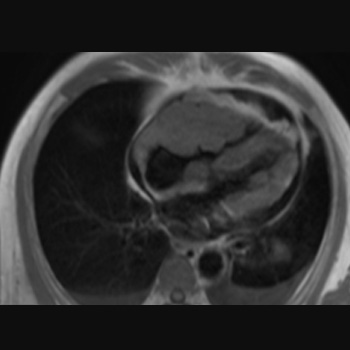
Case presentation: A 66-year-old man with a history of worsening shortness of breath during activity for the last three weeks sought medical attention. The patient later experienced swelling in the extremities, fluid build-up around the lungs and abdominal fluid accumulation, with no reported chest pain, fever, or weight loss. An echocardiogram found a mass in the lateral wall near the tricuspid valve of the right ventricle, leading to moderate tricuspid stenosis. The cardiac magnetic resonance imaging (MRI) revealed a lumpy, poorly defined mass that invaded the heart muscle and displayed varied enhancement after contrast administration. Suspicion arose for a malignant tumour or metastatic lesion due to its features and contrast uptake capability. A percutaneous biopsy was carried out on the mass in the right ventricle to confirm the diagnosis. The pathology report indicated a diagnosis of non-Hodgkin’s lymphoma. After being diagnosed, the patient underwent chemotherapy using the R-CHOP regimen. Over time the symptoms improved, and echocardiograms revealed a decrease in the size of the tumour. After undergoing six rounds of chemotherapy, a cardiac MRI four months later showed no signs of a tumour. After that, the patient resumed their regular activities.
Conclusion: Right ventricular tumours are mostly malignant lesions and often have an inferior prognosis. Early diagnosis with imaging techniques and myocardial biopsy is necessary to deliver life-saving treatment quickly.

|
Views: 957
HTML: 127
PDF: 395
|
Persistent left superior vena cava (PLSVC) is the most common variation of anomalous venous return to the heart and present in 0.1–0.5% of the general population. The left anterior cardinal veins typically obliterate during early cardiac development but failure of involution results in PLSVC. It is an asymptomatic congenital anomaly, usually discovered while performing interventions through the left subclavian vein or during cardiovascular imaging. PLSVC can be associated with cardiac arrhythmias and congenital heart disease. We present two cases of PLSVC: first, a 68-year-old male who presented with complete heart block, for which a temporary pacemaker was initially inserted followed by a permanent pacemaker; second, a 53-year-old female with a history of hypertension and ischemic cardiomyopathy with a left ventricular ejection fraction of 25%, and a survivor of sudden cardiac death, who underwent an implantable cardioverter-defibrillator (ICD) for secondary prevention.
Both cases of PLSVC were detected incidentally during the transvenous approach to the heart. PLSVC was suspected by the unusually left medial position of the lead, while cineflouroscopy showed the venous trajectory toward the coronary sinus and drainage into the right atrium. It is technically difficult to cross the wire through the tricuspid valve when coming from the PLSVC and coronary sinus without making a loop in the right atrium, which is known as a wide loop technique.
PLSVC is an uncommon anomalous anatomical variant and should be recognized appropriately by specialists who frequently carry out procedures through the left subclavian vein, such as implantation of permanent pacemaker, ICD and cardiac resynchronization therapy. It should also be recognized that wide loop formation of the right ventricular lead in the right atrium is helpful to cross the tricuspid valve and to affix the lead in the right ventricle.
|
Views: 1125
HTML: 212
PDF: 900
|
Background: Paliperidone and mirtazapine are psychotropic agents associated with proarrhythmic effects.
Case Presentation: A 21-year-old woman was admitted to the intensive care unit on two separate occasions for attempting suicide by overdosing on paliperidone and mirtazapine. During both admissions, the patient had atypical chest pain and a first-degree atrioventricular block (AVB) with paradoxical sinus tachycardia, which resolved with the discontinuation of paliperidone and mirtazapine and aggressive intravenous fluids.
Conclusion: Drug-induced first-degree AVB from paliperidone and mirtazapine should be on the differential diagnosis in patients on paliperidone and/or mirtazapine who present with chest pain, tachycardia or new-onset first-degree AVB
|
Views: 26
PDF: 27
HTML: 4
|
Background: Studies have shown major cardiovascular effects associated with ketamine use disorder including dose-dependent negative inotropic effects. Preoperative ketamine use has been linked to ketamine-induced stress cardiomyopathy.
Case presentation: A 28-year-old female with a history of recurrent cystitis and ketamine use disorder (twice weekly for 14 years) presented with bilateral lower extremity oedema and shortness of breath for 3 months. She was tachycardic with a troponin level of 0.07 ng/ml and a B-type natriuretic peptide (BNP) level of 2511 pg/ml. Electrocardiogram showed normal sinus rhythm and transthoracic echocardiography (TTE) showed left ventricular ejection fraction (EF) of 15%, dilated left ventricle, and severe tricuspid and mitral regurgitation. Computed tomography (CT) scan of the chest and abdomen showed bilateral pleural effusions with congestive hepatopathy and ascites. The patient was started on intravenous furosemide, metoprolol, and sacubitril/valsartan. Rheumatological workup including complement levels, and antinuclear anti-double-stranded DNA was negative. A repeat TTE 2 weeks later revealed an EF of 25% and moderate tricuspid regurgitation. Four months later, the EF was 54% with normal left ventricular cavity size.
Conclusion: Although ketamine use disorder is increasing, data on long-term side effects is minimal. Screening for ketamine use disorders should be considered in patients presenting with acute systolic heart failure. Long-term studies are needed to evaluate the benefits of adding ketamine screening to standard urine toxicology.
|
Views: 328
HTML: 58
PDF: 221
|
Ofatumumab is a monoclonal antibody used in the treatment of recurrent and progressive chronic lymphocytic leukaemia (CLL) and was recently approved for the treatment of multiple sclerosis.
We describe the case of a 68-year-old man who presented with complaints of irregular pulse readings while undergoing ofatumumab treatment for recurrent CLL. Electrocardiograms (ECGs) demonstrated premature ventricular contractions (PVCs) which eventually caused cardiomyopathy and failed to resolve despite ablative therapy. Ofatumumab-induced PVCs are confirmed in this case by the existence of documented PVCs on ECGs and the disappearance of these PVCs after the completion of ofatumumab treatment.
To the best of our knowledge, there have been no previously reported cases of PVCs associated with ofatumumab in the literature.
|
Views: 458
HTML: 281
PDF: 225
|
Hypoplastic coronary artery disease is a rare congenital anomaly that may present with ischaemic heart disease, heart failure or sudden cardiac death (SCD). We describe a case of cardiac arrest in a healthy young man. Work-up revealed a hypoplastic left anterior descending artery. The patient underwent cardioverter-defibrillator implantation for secondary prevention.
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2023, Published by SMC Media srl, Italy - Privacy policy

