EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 1828
HTML: 320
PDF: 595
Figure 1: 0
Figure 2: 0
|
Chlorpyrifos is an organophosphate compound recognized as causing acute toxicity. However, organophosphate-induced delayed polyneuropathy (OPIDP), although rare, has also been described. We describe an unusual presentation of OPIDP with flaccid quadriplegia progressing to a locked-in-like syndrome, 30 days after a 60-year-old man voluntarily ingested chlorpyrifos. In the absence of specific treatment, the patient only recovered partial motor responses and the ability to communicate. The authors present this report in order to highlight a form of OPIDP which can hinder diagnosis due to its atypia and the delay in the onset of symptoms from initial contact with the toxicant.

|
Views: 1814
HTML: 823
PDF: 543
|
Introduction: Missing a leaking abdominal aortic aneurysm (AAA) is common in medical practice because few at-risk patients have a history of AAA and many have an unusual presentation.
Background: AAA is less common among Asians than white Caucasians of the same age. Our patient had no significant risk factors apart from age and sex and had an unusual presentation.
Patient and Methods: A 67-year-old Asian man presented to the emergency room (ER) with a 1-day history of nausea, vomiting, diarrhoea, fever and abdominal pain. He was febrile, dehydrated. and had marked tenderness at the right iliac fossa. Laboratory findings suggested bacterial gastroenteritis but this did not explain the localized tenderness at the right iliac fossa.
Result and Discussion: A CT scan of the abdomen revealed an AAA arising above the origins of the renal arteries, an intramural thrombus, a retroperitoneal haematoma and a leak extending to the right iliac fossa. The patient was transferred to another hospital and underwent exploratory laparotomy, surgical repair of the aneurysm, and aortobi-iliac grafting with removal of the thrombus. The patient was discharged in good shape 3 weeks after surgery. Without the CT scan of the abdomen, the AAA could have been missed and the patient treated for severe gastroenteritis.
|
Views: 3012
HTML: 283
PDF: 2369
|
This case demonstrates the therapeutic challenges encountered when managing an acute pulmonary embolism in a cancer patient with thrombocytopenia. A 64-year-old man with a history of lung cancer receiving chemotherapy was admitted to Walsall Manor Hospital with haemodynamic instability consistent with a pulmonary embolism, proven on computed tomographic pulmonary angiogram. His platelet count was noted to be 35×109/l (chemotherapy-induced thrombocytopenia). After discussions, he was deemed not suitable for thrombolysis based on risk versus benefits. The patient was initially transfused one adult dose of platelets and treated with half the therapeutic dose of low molecular weight heparin (LMWH). The same management plan was followed until the platelet count exceeded 50×10sup>9/l, after which the patient was established on the full therapeutic dose of LMWH. Clinically, the patient improved and was discharged. Three months after discharge, follow-up revealed sustained clinical improvement while the patient continued to be on the full therapeutic dose of LMWH with a stable platelet count.

|
Views: 3334
HTML: 487
pdf: 639
|
A 46-years old woman presented with acute onset of nausea, vomiting and prostration in the ER. She appeared ill and was poorly responsive to verbal stimuli. The physical examination showed a systolic blood pressure of 60 mmHg and a pulse of 40 bpm. ECG was notable for slight ST-elevations in the inferior leads. Right ventricular myocardial infarction with cardiogenic shock and bradycardia was suspected. Supportive therapy with catecholamines was initiated and a emergency coronary angiography was arranged. However, lab results showed normal troponin levels and a subsequent echocardiogram showed the absence of abnormal wall motions. By thorough history taking with the spouse it turned out that the patient had consumed a Turkish honey approximately an hour before the beginning of the symptoms. The patient made a full recovery within 24 hours with only supportive therapy. In retrospect the clinical presentation was highly indicative of poisoning with Grayanotoxins from a plant, Rhododendron, which is found as contaminant in some sorts of honey in the Black Sea area. A pollen analysis confirmed the presence of Rhododendron in a honey sample. Historically this poisoning is mentioned over the millennia as mad honey disease. The ST-elevations in the ECG were a sign of early repolarization, a non-pathological finding.
|
Views: 1404
HTML: 1305
PDF: 542
|
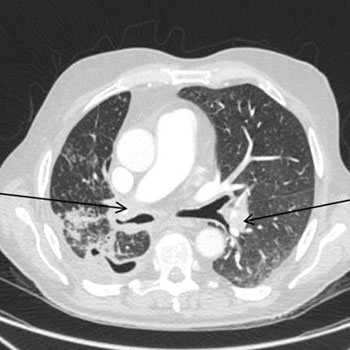
An 84-year-old woman had five episodes of pneumonia in 4 months. Despite extensive comorbidities and advanced age, her health status was good and the recurrence seemed unjustified. Exhaustive background investigation revealed 14 episodes of right-sided pneumonias during the 3 previous years and an inconclusive investigation with CT of the thorax and bronchofibroscopy, despite some fibrotic and atelectasic alterations in the right middle lobe. A new right-sided x-ray showed a wedge-shaped density extending anteriorly and inferiorly from the hilum, and CT of the thorax revealed aggravated middle lobe abnormalities with thickening of the bronchial wall and segment atelectasis, without any visible airway obstruction. After extensive work-up had excluded other causes of recurrent pneumonia and immunodeficiency, a non-obstructive middle lobe syndrome (MLS) was deemed responsible for the repeated episodes of pneumonia. MLS is characterised by chronic hypoventilation and atelectasis of the middle lobe, facilitating secretion accumulation, chronic inflammation and repeated infection. After treatment with bronchodilators and immunostimulants was initiated, the patient experienced no recurrences for several months.
|
Views: 1406
HTML: 312
PDF: 757
|
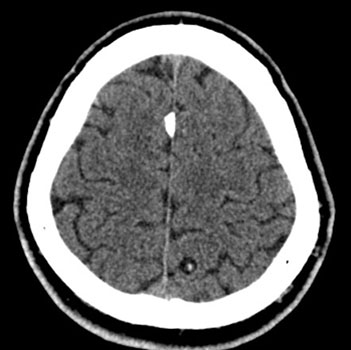
Cysticercosis is triggered by infection with the larval form of the tapeworm Taenia solium. The usual sites for the development of cyscticerci are the central nervous system (neurocysticercosis – NCC), subcutaneous tissue, skeletal muscle, heart muscle, and the eye. Ocular cysticercosis is caused by the growth of the larvae within ocular tissues. The extraocular muscles form is the most common type of orbital cysticercosis. We report a case of a patient admitted with seizures secondary to NCC, who developed ocular symptoms after starting combined treatment with albendazole, praziquantel and dexamethasone. The investigation revealed a cystic lesion in the lateral rectus muscle.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

