EJCRIM 2023 CiteScore
| 2.1 = | 1.751 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by




|
Views: 9
HTML: 1
PDF: 4
|
Euglycemic diabetic ketoacidosis (euDKA) is a rare but severe metabolic complication of diabetes mellitus characterised by elevated anion gap metabolic acidosis despite normal or mildly elevated blood glucose levels. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have emerged as effective antidiabetic medications, yet their use is associated with an increased risk of euDKA, especially when coupled with insulin dose reduction.
We present the case of a 50-year-old male with a 20-year history of diabetes mellitus, initially managed with insulin and metformin, who developed euDKA following the introduction of empagliflozin and sitagliptin alongside a reduction in insulin therapy. Despite normoglycaemia the patient exhibited symptoms of ketoacidosis, including chronic fatigue, polydipsia, and polyuria.
Diagnostic workup revealed metabolic acidosis, elevated inflammatory markers, acute kidney injury and ketonuria. Subsequent specialised laboratory tests confirmed type 1 diabetes mellitus (T1DM) with the presence of anti-glutamic acid decarboxylase (anti-GAD) antibodies and the absence of C-peptide secretion. Management involved fluid therapy, intravenous insulin and glucose administration.
This case underscores the diagnostic challenges of euDKA and emphasises the importance of differentiating between T1DM and T2DM, as management strategies vary significantly. Patient education on insulin therapy and injection techniques is crucial to prevent complications such as improper insulin delivery and dose reduction, which can precipitate euDKA.
In conclusion, clinicians should be vigilant for euDKA in patients on SGLT2 inhibitors, particularly when insulin dose reduction is involved. Comprehensive patient education and accurate differentiation between diabetes types are essential for timely diagnosis and optimal management, thereby reducing the risk of severe complications.
|
Views: 72
HTML: 7
PDF: 51
|
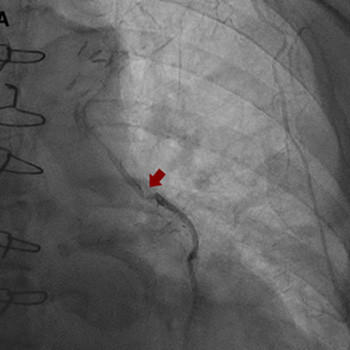
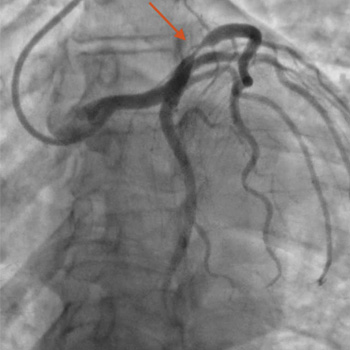
Intracoronary in-stent restenosis (ISR) is a phenomenon that generally occurs between 3 and 6 months after stent placement. With the introduction of drug-eluting stents (DES), the incidence of ISR has decreased but not disappeared. We report a case of reiterant in-stent restenosis of an 81-year-old female patient who underwent multiple percutaneous coronary intervention and two coronary artery bypass surgeries. ISR is possibly associated with extra-stent, stent-related and intra-stent factors. Here, we excluded the first two and focused on the intra-stent factors that seem more likely in our case. A challenging diagnostic workup led us to the hypothesis of a coronary vasculitis potentially triggered by some component of the stent in a predisposed patient carrier of non-disease-specific ANA, with an exaggerated immune response. No recurrence of ISR occurred after the introduction of steroids. Biological and intra-stent causes of ISR should be taken into careful consideration to aim for the early detection of the underlying mechanism of restenosis and to embrace the best therapeutic strategy.
|
Views: 95
HTML: 5
PDF: 84
|
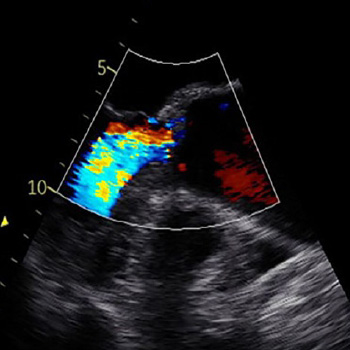
Case description: We describe a case of a patient treated with pembrolizumab (an immune checkpoint inhibitor) for metastatic scalp melanoma. He had a previous history of colorectal cancer, prostatic cancer and chronic polymyalgia rheumatica. The patient was known to have a stable ascending aortic aneurysm of 4.5 cm. However, he developed a rapid expansion of the ascending aortic aneurysm with the size crossing the threshold for surgery. The patient was referred to the cardiothoracic surgery service for intervention and he subsequently underwent surgery. The patient was electively admitted one week later for resection of aortic aneurysm, aortoplasty and external graft fixation. Pathologically, gross evidence of dissection was not identified; however, the histological analysis of the media showed laminar medial necrosis, multifocal in nature, with occasional clusters of histiocytic cells appreciated at their edge reminiscent of that seen in an inflammatory aortitis (granulomatous/giant cell type).
Discussion: Immune checkpoint inhibitor-induced aortitis is becoming increasingly evident, and its presentation can vary. It has been discovered incidentally on surveillance imaging with the use of nivolumab. In other cases, patients have been symptomatic to severely symptomatic. Atezolizumab with carboplatin and etoposide has been reported to cause abdominal aortitis which was responsive to corticosteroids and subsequent discontinuation of atezolizumab. Pembrolizumab has been linked to a case of transverse aortic arch aortitis. In our case, the inflammatory aortitis due to pembrolizumab was the cause of the rapid expansion of the ascending aortic aneurysm.
Conclusion: Patients with known aortic aneurysms should undergo careful surveillance when commencing immune-checkpoint inhibitor therapy.
|
Views: 101
HTML: 11
PDF: 74
|
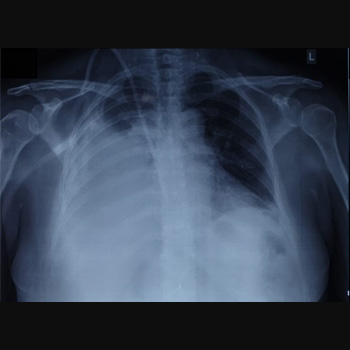
Pleuroperitoneal leak as a cause of pleural effusions in peritoneal dialysis is a rare but important complication to consider in continuous ambulatory peritoneal dialysis (CAPD) patients presenting with recurrent progressive dyspnoea. Generally, these effusions are unilateral and right-sided, resulting in shortness of breath and reduced ultrafiltration volume, which are initially managed by peritoneal rest. We describe a case of bilateral pleural effusions in a 57-year-old female on chronic CAPD who developed recurrent progressive dyspnoea but maintained adequate dialysis output. A chest radiograph revealed bilateral pleural effusions with high glucose content, and scintigraphy confirmed the existence of a definite pleuroperitoneal communication. She was managed by temporary substitution to haemodialysis, followed by suturing of the shunt and successful video-assisted thoracoscopic surgery (VATS) pleurodesis with an aldehyde-based surgical glue. Unexplained recurring dyspnoea in chronic CAPD should raise the suspicion of a possible pleuroperitoneal leak, even in patients without an apparent loss of ultrafiltration. Pleurodesis using an aldehyde-based adhesive was effective and tolerated well by our patient and may be considered in managing cases of recurrent pleural effusion.
|
Views: 233
HTML: 30
PDF: 156
|
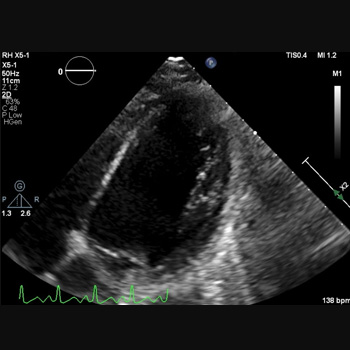
Introduction: Combination-based adjuvant chemotherapy utilising capecitabine and oxaliplatin is widely used in gastric cancer treatment. Rare but severe cardiac events such as prolonged QT, cardiac arrest and cardiogenic shock can result from their use.
Case description: A 45-year-old female with gastric adenocarcinoma was started on capecitabine-oxaliplatin chemotherapy one week before presenting to the emergency department with weakness. Blood pressure was 78/56 mmHg, heart rate 140 bpm and oxygen saturation 85%. She became unresponsive with pulseless ventricular fibrillation; CPR was initiated with immediate intubation. She received two shocks with a return of spontaneous circulation. Laboratory tests revealed serum potassium (3.1 mmol/l), magnesium (1.1 mg/dl) and troponin (0.46 ng/ml). An EKG revealed sinus tachycardia with a prolonged QT interval (556 ms). The combined effects of capecitabine, oxaliplatin and electrolyte abnormalities likely contributed to the QT prolongation. An echocardiogram demonstrated an ejection fraction of 10%–15%. An emergent right-heart catheterisation showed right atrial pressure of 10 mmHg and pulmonary artery pressure of 30/18 mmHg; cardiac output and index were not recorded. An intra-aortic balloon pump was placed, and she was admitted to the ICU for cardiogenic shock requiring norepinephrine, vasopressin and dobutamine. A repeat echocardiogram showed a significantly improved ejection fraction of 65%, and she was discharged.
Discussion: Capecitabine and oxaliplatin cardiotoxicity is an exceedingly rare occurrence, with both drugs reported to cause QT prolongation.
Conclusion: Healthcare providers must recognise the QT prolongation effects of capecitabine and oxaliplatin, leading to life-threatening cardiac arrhythmias.
|
Views: 177
HTML: 13
PDF: 154
|
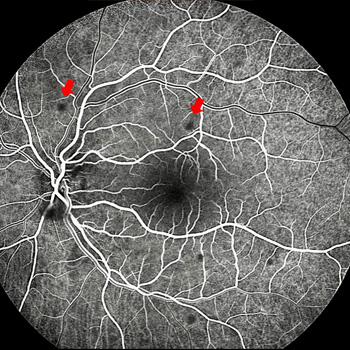
Introduction: A case of ocular bartonellosis under anti-tumour necrosis factor treatment is described.
Case description: A 29-year-old woman with psoriasis who had been on certolizumab treatment was examined with a left visual deterioration following a fever bout, malaise, and placoid erythematous rashes on her neck. As there was acute anterior uveitis in her left eye, it was recommended to stop certolizumab treatment for a possible infectious aetiology. However, her physician elected to continue the certolizumab treatment. Ten days later, the patient noticed further visual decline despite the topical steroid treatment. This time, there were scattered yellow-white small retinitis foci at the left posterior pole. Infectious agents were searched and while Bartonella henselae antibodies were negative for immunoglobulin M, the immunoglobulin G titre was 1/80. Clinical findings were improved with the systemic treatment of oral trimethoprim-sulfamethoxazole (160/800 mg twice daily for six weeks) and azithromycin (500 mg once daily for two weeks).
Discussion: Though extremely rare, ocular bartonellosis should be kept in mind in patients on anti-tumour necrosis factor treatment as rapid and accurate diagnosis may end up with an excellent visual outcome and full recovery.
|
Views: 224
HTML: 28
PDF: 242
|
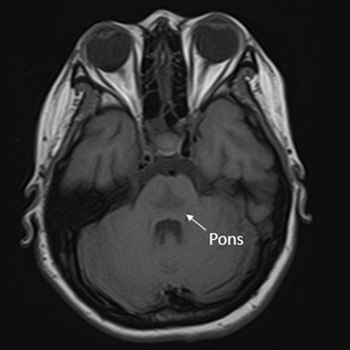
Osmotic demyelination syndrome (ODS) is a disorder characterised by the widespread development of demyelination in both pontine and extrapontine regions. It has been recognised as a complication arising from the rapid correction of hyponatraemia. This study presents the case of a 20-year-old Thai female patient at 10 weeks gestation, exhibiting an initial presentation of catatonia – an uncommon manifestation of ODS. The patient developed symptoms following the rapid correction of hyponatraemia in the context of hyperemesis gravidarum. Magnetic resonance imaging (MRI) of the brain revealed a trident or bat-wing-shaped pattern in T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences at the central pons. The patient underwent five cycles of plasmapheresis and received rehabilitation, leading to clinical improvement.

|
Views: 260
HTML: 30
PDF: 160
|
Background: This report presents the influence of immunosuppression by new rheumatological therapies on hepatitis E virus infection in a 54-year-old male patient with an anti-synthetase syndrome and treatment with methotrexate and rituximab.
Case description: The patient arrived at the Emergency Department with epigastric pain, vomiting and dark urine. Initial examination revealed signs of inflammation and hepatic dysfunction. Subsequent laboratory tests and imaging confirmed acute hepatitis E infection in the context of recent initiation of rituximab therapy. Despite initial suspicion of pancreatitis, subsequent investigations ruled out pancreatic involvement. Treatment with ribavirin, along with supportive measures, led to significant clinical improvement with resolution of jaundice, ascites, and oedema.
Conclusions: This case underscores the importance of considering hepatitis E in patients with autoimmune conditions, especially when initiating immunosuppressive therapies, a situation that is not well described in scientific literature and is increasingly common, necessitating proper recognition.
|
Views: 474
PDF: 284
HTML: 11
|
Introduction: During treatment for malignant lymphoma, cytopenia can develop for several reasons. This can range from mild cytopenias leading to infection and bleeding to full-blown drug-induced aplastic anaemia. While aplastic anaemia affects individuals of all genders and ages, here, we describe aplastic anaemia after chemotherapy exposure to bendamustine in a 65-year-old female with non-Hodgkin’s lymphoma.
Case description: A 65-year-old woman with recurrent indolent marginal zone lymphoma and post-chemotherapy with bendamustine and rituximab, presented with a neutropenic fever and was admitted with a leading diagnosis of sepsis. In the previous two weeks, the patient required regular transfusions of packed red blood cells and platelets and maintained a daily ZARXIO® regimen. Laboratory results revealed pancytopenia, and broad-spectrum antibiotics (cefepime/vancomycin) were given. The patient was subsequently admitted to the hospital under the care of the haematology/oncology team and was ultimately diagnosed with aplastic anaemia, likely as a consequence of bendamustine chemoimmunotherapy. She elicited a positive response to the triple immunosuppressive therapy (IST) regimen (two immunotherapeutic agents plus one anti-thymocyte globulin (ATG), after which her cell counts returned to normal.
Conclusions: This case underscores the importance of recognising haematologic complications linked to bendamustine and advocates for further research to increase the understanding among healthcare professionals of drug-induced aplastic anaemia. Bendamustine can cause severe autoimmune haemolytic anaemia and aplastic anaemia and may require multiple transfusions and a multidrug regimen for treatment. The use of ATG as a therapeutic intervention is appropriate because it has been effective in treating aplastic anaemia.
|
Views: 303
HTML: 14
PDF: 172
|
Anagrelide is a medication primarily used to manage thrombocytosis, an abnormal increase in platelet levels in the blood. It is often prescribed for patients with myeloproliferative disorders, such as essential thrombocythaemia (ET). Given the heightened susceptibility to thromboembolism associated with this condition, the primary emphasis in treatment revolves around reducing the risk of thrombotic events through the administration of cytotoxic agents. While anagrelide is generally effective in reducing platelet counts, it comes with potential side effects, including an increased risk of certain thrombotic events. Anagrelide acts by inhibiting megakaryocyte maturation and platelet release, thereby reducing platelet production. However, this platelet-lowering effect may be accompanied by an increase in platelet activation and reactivity, which could contribute to a prothrombotic state. We present a case of a 60-year-old female with a history of ET, managed with anagrelide and hydroxyurea therapy, who experienced an acute ST-elevation myocardial infarction.
| 2.1 = | 1.751 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

