EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 1579
HTML: 891
PDF: 728
|
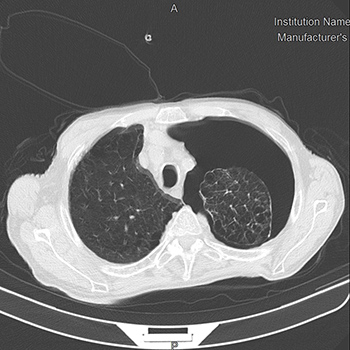
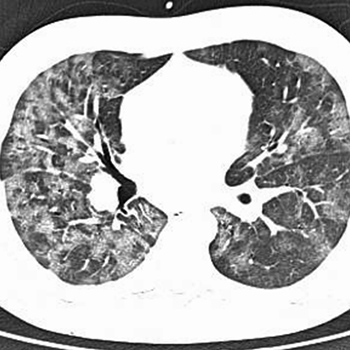
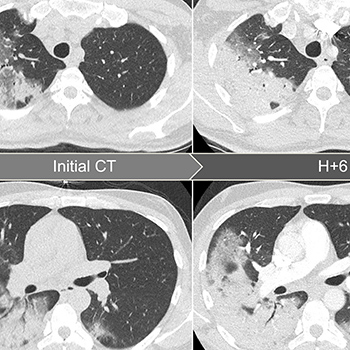
We describe the case of a male patient admitted to our emergency department during the Italian COVID-19 epidemic, for progressive worsening dyspnoea. A diagnosis of pneumothorax and diffuse interstitial lung involvement was promptly made by lung ultrasound and confirmed by an HRCT scan. A chest CT scan also showed diffuse emphysema, as observed in chronic obstructive pulmonary disease (COPD), and small consolidations in the lower lobes, suggestive for COVID-19 pneumonia. A chest tube was immediately inserted in the emergency room with complete resolution of the dyspnoea. A nasopharyngeal swab for 2019-nCoV was positive. Unfortunately, the patient died from COVID-19-related acute respiratory distress syndrome after 48 days of hospitalization.
|
Views: 4908
HTML: 421
PDF: 1233
|
The literature suggests that COVID-19 provokes arterial and venous thrombotic events, although the mechanism is still unknown. In this study, we describe patients with confirmed coronavirus infection associated with multisystemic infarction, focusing on splenic infarction. More data are required to elucidate how COVID-19 and thrombotic disease interact and so that preventive and early diagnosis strategies can be developed.
|
Views: 977
HTML: 97
PDF: 513
|
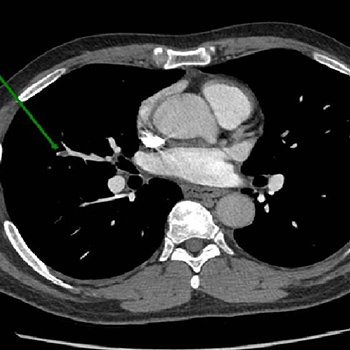
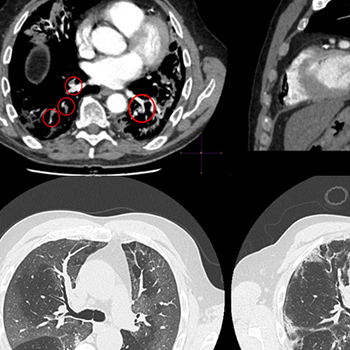
Thromboembolic disease is strongly associated with, or even an integral part of, COVID-19 pneumonia. Indeed, endothelial/microvascular damage to pulmonary capillaries seems to be the main trigger of the pneumonia. Here we report a case of pulmonary embolism in a COVID-19 patient with an atypical clinical presentation. Blood gas analysis and lung ultrasound allowed the correct diagnosis to be reached.
|
Views: 1266
HTML: 318
PDF: 528
|
We described three COVID-19-infected patients with profound immune thrombocytopenia causing haemorrhagic mucocutaneous complications. We conclude that an immune mechanism was responsible as common causes were excluded. Since corticoids were considered harmful in the circumstances, the patients were successfully treated with intravenous immunoglobulins without later relapse.

|
Views: 1693
HTML: 3805
PDF: 722
|
COVID-19 is the clinical expression of the highly contagious severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral infection. Most patients have mild symptoms, but a significant proportion have severe or critical disease, which can include cardiac injury, sepsis, acute kidney failure and respiratory failure. It is also worth highlighting the increasing number of reported COVID-19 cases with dermatological disease/manifestations. The cutaneous clinical spectrum is wide and includes maculopapular, urticarial, varicelliform and petechial rashes, pseudo perniosis, livedo reticularis, and pityriasis rosea-like, violaceous and pustular lesions. Until the physiological mechanism is fully understood, it is important to describe these manifestations, which could help identify a typical pattern. This report describes a cutaneous manifestation in a COVID-19 patient.
|
Views: 1056
HTML: 111
PDF: 605
|
Infection with SARS-CoV-2 causes critical disease in approximately 5% of affected patients, particularly the elderly, hypertensive, obese and immunocompromised. Patients with haematological cancer, including chronic lymphocytic leukaemia (CLL), are particularly at risk of complications. Very rarely, patients with extreme leukocytosis may develop spurious hypoxemia, or pseudohypoxemia, which confuses the diagnosis of complications and can lead to intervention errors. We report the case of a patient with CLL, severe infection with SARS-CoV-2 and pseudohypoxemia.
|
Views: 1092
HTML: 127
PDF: 761
|
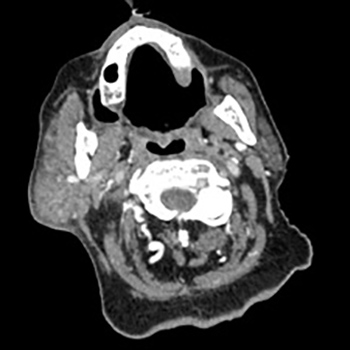
We describe the case of a patient hospitalized for acute decompensated heart failure in a standard medical ward. During hospitalization, he was diagnosed with COVID-19 and transferred to a special unit. The clinical course was marked by worsening of the respiratory disease, the development of right parotiditis and thrombosis of the left internal jugular vein. Therapeutic anticoagulation was initiated and 2 days later, the minimal dermatoporosis lesions previously present in the upper extremities evolved to haemorrhagic bullae with intra-bullae blood clots and dissecting haematomas. Surgical management of the dissecting haematomas was difficult in the context of haemostasis abnormalities. The patient died 29 days after hospital admission.
|
Views: 8322
HTML: 411
PDF: 1599
|
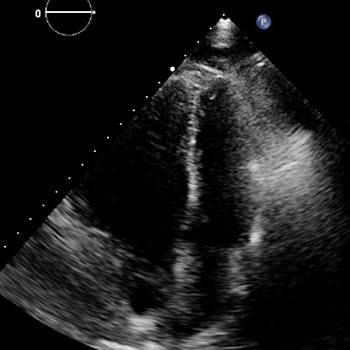
COVID-19 is a novel viral disease caused by SARS-CoV-2. The mid- and long-term outcomes have not yet been determined. COVID-19 infection is increasingly being associated with systemic and multi-organ involvement, encompassing cytokine release syndrome and thromboembolic, vascular and cardiac events. The patient described experienced unusually rapid development of pulmonary hypertension (PH) and right ventricular failure after recent severe COVID-19 pneumonia with cytokine release syndrome, which initially was successfully treated with methylprednisolone and tocilizumab. The development of pulmonary hypertension and right ventricular failure – in the absence of emboli on multiple CT angiograms – was most likely caused by progressive pulmonary parenchymal abnormalities combined with microvascular damage of the pulmonary arteries (group III and IV pulmonary hypertension, respectively). To the best of our knowledge, these complications have not previously been described and therefore awareness of PH as a complication of COVID-19 is warranted.
|
Views: 1540
HTML: 1126
PDF: 649
|
Introduction: SARS-CoV-2 infection may predispose patients to thrombotic disease. Patients with COVID-19 pneumonia who are receiving non-vitamin K antagonists or direct oral anticoagulants for chronic disease are usually switched to heparin treatment during hospitalization. However, information about the most appropriate antithrombotic therapy after the acute infection phase is lacking.
Case Description: We report the case of a patient with chronic atrial fibrillation who was recently hospitalized for severe COVID-19 pneumonia. Four weeks after discharge he experienced an episode of an acute pulmonary embolism while on rivaroxaban therapy with adequate drug plasma levels, and in the absence of strong predisposing risk factors.
Conclusion: This case highlights the risk of thrombotic complications after COVID-19 infection, raises some concern about their underlying mechanisms, and supports the use of effective anti-thrombotic therapy.

|
Views: 930
HTML: 162
PDF: 416
|
Patients with COVID-19 pneumonia can develop heart problems and may also may be susceptible to proarrhythmia, virus-related issues such as fever, stress, electrolyte disturbance and adverse effects from the use of antiviral drugs. We report a transient Brugada-like ECG pattern without ongoing fever in a 57-year-old man, admitted with a diagnosis of COVID-19 pneumonia, who did not have syncope or a family history of sudden cardiac death.
|
Views: 673
HTML: 285
PDF: 381
|
Background: In June 2020, a large randomised controlled clinical trial in the UK found that dexamethasone was effective in reducing the number of deaths in patients with severe coronavirus disease 2019 (COVID-19).
Case description: We describe a patient with rapid worsening of COVID-19 pneumonia and its dramatic improvement under corticosteroids.
Discussion: Corticosteroids could be useful in patients with an inflammatory profile, considering that acute respiratory distress syndrome may be the consequence of cytokine storm syndrome.

|
Views: 2099
HTML: 6209
PDF: 683
|
Non-polio enteroviruses are ubiquitous viruses responsible for a wide spectrum of disease in people of all ages, although infection and illness disproportionately affect infants and young children. Hand-foot-mouth disease (HFMD) is an enteroviral clinical syndrome most frequently caused by coxsackievirus-A16 and enterovirus-A71. Since 2008, a novel coxsackievirus-A6 genotype has been associated with more severe HFMD in both children and adults, presenting with a unique constellation of findings, and whose prevalence has been increasing over the last few years. In this case report, an atypical clinical picture of confirmed enterovirus HFMD is described in an immunocompetent adult, with exuberant clinical findings, clinically consistent with coxsackievirus-A6 infection. This case report highlights the importance of awareness of the clinical presentation of this increasingly common infection in adults.
|
Views: 999
HTML: 203
PDF: 444
|
Patients with Strongyloides stercoralis infections are usually asymptomatic but massive hyperinfection may occur in patients with diseases associated with abnormal cell-mediated immunity or receiving immunosuppressive therapy.
The authors present the clinical case of a 49-year-old man with a history of diarrhoea and cramping abdominal pain, generalized oedema, petechial rash, melanoderma, cough and dyspnoea. He presented hypokalaemia and arterial hypertension and was admitted with the diagnostic hypothesis of Cushing’s syndrome or adrenocorticotropic hormone ectopic production. The patient developed respiratory failure associated with bilateral lung opacities and was admitted to the Intensive Care Unit. The abdominal computed tomography scan revealed liver and duodenal masses. The duodenal biopsy showed the presence of Strongyloides stercoralis and the liver biopsy showed the presence of small cell neuroendocrine carcinoma. The patient died 50 days after hospital admission. The high level of endogenous cortisol observed in this patient may have facilitated the progression to severe fatal infection.
|
Views: 1533
HTML: 2869
PDF: 512
|
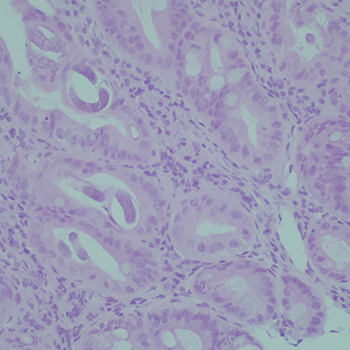
Lisinopril is an angiotensin converting enzyme inhibitor (ACE-I) that has been on market for more than 25 years. ACE-I are usually well tolerated and rarely have serious or life-threatening side effects. We describe an unusual presentation of fulminant hepatic cholestasis probably secondary to lisinopril. To our knowledge, this is the second case report which shows lisinopril-induced liver injury though a cholestatic mechanism. The patient was a 59-year-old woman with type 2 diabetes, a high body mass index and hypertension, who presented with a 5-week history of jaundice and itching. She had been started on lisinopril for diabetic nephropathy 8 weeks before admission. Other causes for cholestasis had been excluded through non-invasive immunology and virology screening, an ultrasound of the liver, magnetic resonance cholangiopancreatography and a liver biopsy. The biopsy was consistent with drug-induced liver injury. Lisinopril was stopped 2 weeks before admission. The patient’s hospital stay was complicated by contrast nephropathy and influenza A which were both treated appropriately. Unfortunately, the liver cholestasis did not completely resolve following withdrawal of lisinopril and the patient died after 4 months. A literature search yielded only six other reported cases of lisinopril-induced liver injury. Five cases described hepatocellular damage and one showed cholestatic injury.
|
Views: 3357
HTML: 1069
PDF: 4108
|
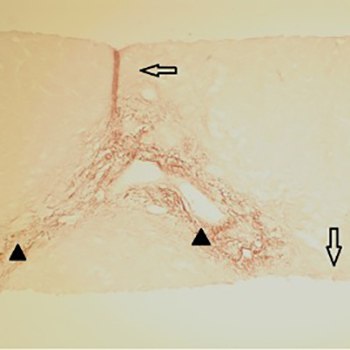
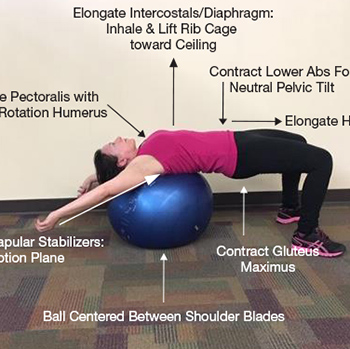
We present a 53-year-old female patient with median arcuate ligament syndrome (MALS), also known as Dunbar syndrome or celiac artery compression syndrome, related to lumbar lordosis and hip dysplasia. She utilized interprofessional management strategies, which were beneficial in reducing lumbar lordosis and MALS-related symptoms. This finding is important because there are no other reports in the literature describing interprofessional strategies to manage symptoms for patients who are waiting for surgery or are not candidates for surgery.

|
Views: 1058
HTML: 178
PDF: 358
|
Right-sided Bochdalek hernia (BH) is very rarely diagnosed in adults. It commonly presents with gastrointestinal symptoms (pain, abdominal distension and vomiting). Breathlessness, recurrent chest infections and other pulmonary sequelae can also be present. We report the case of a 92-year-old man with a 3-day history of dyspnoea, fever and thoracic pain and multiple episodes of vomiting. An x-ray was performed, and the diagnosis of a large BH hernia was confirmed by computed tomography of the thorax. The condition may be fatal in cases where the small bowel undergoes necrosis or perforation. An emergent laparotomy was performed, but the patient did not improve clinically and died immediately after the procedure.
|
Views: 1281
HTML: 187
PDF: 665
|
Infection with cytomegalovirus (CMV) with resistance to ganciclovir (GCV) is a therapeutic challenge in kidney transplant patients, because standard treatment options are nephrotoxic. We report the case of a kidney transplant recipient with GCV-resistant CMV disease, in whom letermovir, a novel inhibitor of CMV packaging, was administered off-label and prevented a relapse of disease once the CMV load was decreased by cidofovir. Furthermore, we observed significant drug interactions between letermovir and tacrolimus.
|
Views: 1564
HTML: 101
PDF: 473
|
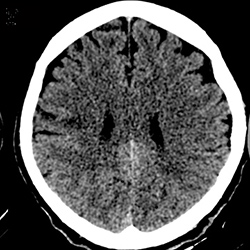
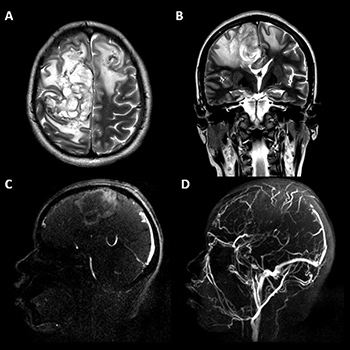
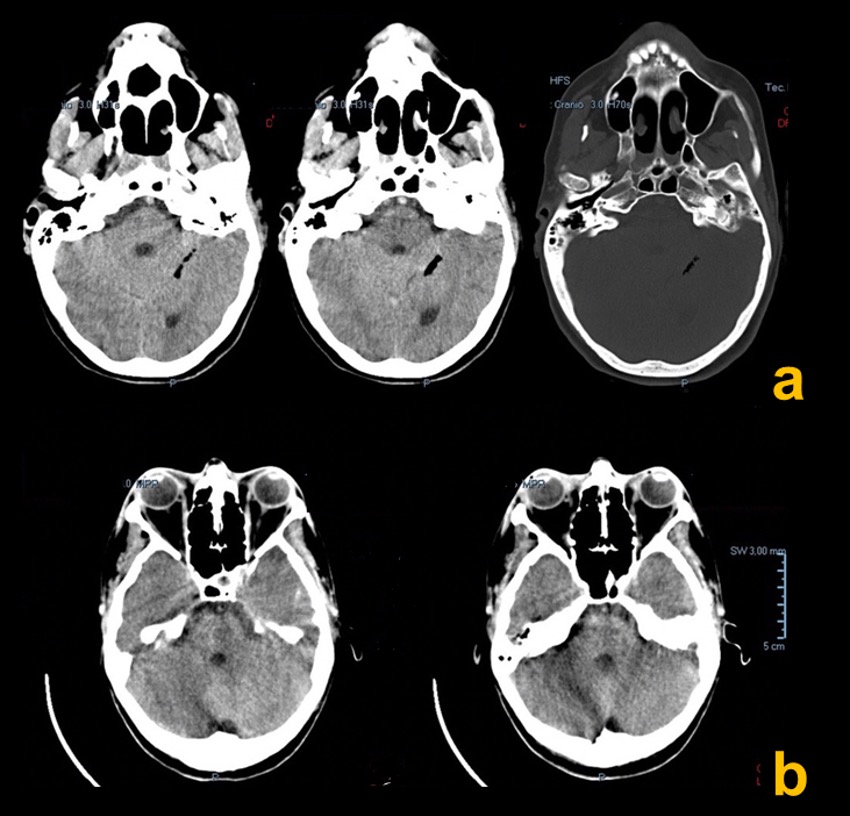
Introduction: Despite the extremely favourable prognosis of patients with cerebral venous thrombosis (CVT), death occurs in 10–15% of patients. In severe cases of malignant CVT with supratentorial haemorrhagic lesions, cerebral oedema and brain herniation, decompressive surgery may be the only life-saving treatment.
Patient and methods: We present the case of a puerperal young woman with progressive headache, seizures and decreased alertness. Thrombosis of the entire superior sagittal sinus with bifrontal venous infarcts and midline shift was confirmed by magnetic resonance imaging with venography sequencing. Despite medical treatment with anticoagulation, progressive neurological deterioration was observed, so bilateral, frontal decompressive craniectomy was performed.
Results: At the 6-month follow-up, we observed partial functional recovery with a modified Rankin score of 3.
Discussion: Bilateral decompressive craniectomy may be a life-saving therapeutic option when medical therapy fails and there are clinical and radiological features of progression in both cerebral hemispheres.

|
Views: 1010
HTML: 157
PDF: 409
|
This report describes the management of a patient with myxoedema coma masquerading as an acute stroke (with or without ‘cold sepsis’). Myxoedema coma is an endocrine emergency occurring when physiological adaptations to untreated hypothyroidism are overwhelmed by an acute precipitant. Even promptly treated, it has an associated mortality of up to 50%.
|
Views: 1138
HTML: 150
PDF: 526
|
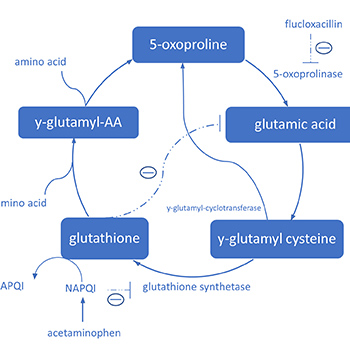
Acetaminophen and flucloxacillin both interfere with the ?-glutamyl cycle. Long-lasting concomitant use of flucloxacillin and acetaminophen can lead to 5-oxoproline accumulation and severe high anion gap metabolic acidosis. Females and patients with sepsis, impaired kidney and/or liver function, malnutrition, advanced age, congenital 5-oxoprolinase deficiency and supratherapeutic acetaminophen and flucloxacillin dosage are associated with increased risk. Therefore, a critical attitude towards the prescription of acetaminophen concomitant with flucloxacillin in these patients is needed.
We present the case of a 79-year-old woman with severe 5-oxoprolinaemia after long-lasting treatment with flucloxacillin and acetaminophen, explaining the toxicological mechanism and risk factors, and we make recommendations for acetaminophen use in patients with long-lasting flucloxacillin treatment.

|
Views: 842
HTML: 179
PDF: 387
|
A 40-year-old man presented to the emergency room and was evaluated in the internal medicine department for unexplained weight loss, asthenia, anorexia and night sweats over the previous 2 months. After a loculated pleural effusion was identified on thoracic computed tomography, purulent fluid was drained from the lung and Fusobacterium nucleatum was isolated. The patient was successfully treated for 27 days with amoxicillin-clavulanic acid. This was an atypical presentation of a common micro-organism implicated in lung infections.
|
Views: 806
HTML: 143
PDF: 341
|
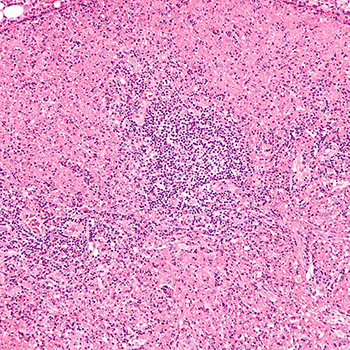
Introduction: Kikuchi-Fujimoto disease (KFD) is a rare, benign, necrotizing lymphadenitis of unknown aetiology with good prognosis. It is characterized by cervical lymphadenopathy, nocturnal diaphoresis and fever. Surgical excision of the adenopathy, histopathological study and immunophenotyping are crucial for diagnosis.
Patients and methods: This paper describes five patients with three different histological subtypes of KFD, including an atypical presentation masquerading as pyelonephritis and two other cases where physicians mistakenly started chemotherapy. In one other case cytomegalovirus was identified as the responsible aetiological agent, while in the remaining patient, KFD evolved into an autoimmune condition.
Discussion: KFD, although rare, may mimic infectious, autoimmune and neoplastic diseases. It also poses a risk for the subsequent development of an autoimmune disorder.
|
Views: 776
HTML: 115
PDF: 422
|
A 44-year-old woman presented with headache and delirium. Brain tomography indicated pneumocephalus, while blood and cerebrospinal fluid cultures revealed Streptococcus pneumoniae. Despite antibiotic treatment and admission to the intensive care unit, the patient died 3 days later. Pneumocephalus in association with meningitis is very rare and may be caused by gas produced by microorganisms.
|
Views: 785
HTML: 117
PDF: 353
|
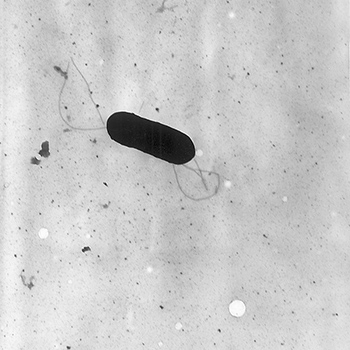
Listeria monocytogenes is a gram positive bacillus responsible for listeriosis. This infection manifests mainly as bacteremia and / or central nervous system (CNS) infection. Involvement of other sites is rare. Pleural listeriosis is an uncommon presentation of L. monocytogenes infection and there is little data to guide the management of these patients. First-line antibiotics used empirically to treat bacterial respiratory infections are ineffective in treating these L. monocytogenes infections, which contributes to the progression of the infection and a worse prognosis.
We present a case report of a patient admitted to an intensive care unit with septic shock secondary to systemic listeriosis with L. monocytogenes isolation in pleural fluid culture and blood cultures. The evolution of the hospitalization and the clinical outcome are reported.
|
Views: 876
HTML: 903
PDF: 464
|
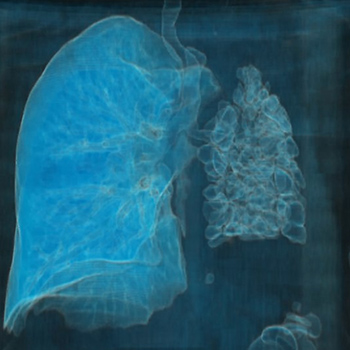
Pulmonary hypoplasia or agenesis is a rare congenital disorder that results in lung underdevelopment. This disease is usually found in children but rarely encountered in adults. We describe the case of an 84-year-old woman diagnosed with a unilateral pulmonary hypoplasia presenting simultaneously with left pulmonary artery hypoplasia. Due to this condition, the patient had a lifelong history of pulmonary infections that resulted in several bronchiectases in the affected lung. Moreover, the pulmonary artery hypoplasia led to the development of pulmonary hypertension and collateral circulation causing hemoptysis, giving rise to the patient attending the emergency department. Although we were able to medically manage the hemoptysis, it can be fatal and require surgical intervention. Hence, an early diagnosis is essential so that appropriate follow-up and prompt prevention and treatment of complications, such as pulmonary infections, hemoptysis and pulmonary hypertension, are achieved.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

